

Developing and validating the model of tumor-infiltrating immune cell to predict survival in patients receiving radiation therapy for head and neck squamous cell carcinoma
- PMID: 38410204
- PMCID: PMC10894341
- DOI: 10.21037/tcr-23-2345
Developing and validating the model of tumor-infiltrating immune cell to predict survival in patients receiving radiation therapy for head and neck squamous cell carcinoma
Abstract
Background: Radiotherapy (RT) is a mainstay of head and neck squamous cell carcinoma (HNSCC) treatment. Due to the influence of RT on tumor cells and immune/stromal cells in microenvironment, some studies suggest that immunologic landscape could shape treatment response. To better predict the survival based on genomic data, we developed a prognostic model using tumor-infiltrating immune cell (TIIC) signature to predict survival in patients undergoing RT for HNSCC.
Methods: Gene expression data and clinical information were downloaded from The Cancer Genome Atlas (TCGA) and Gene Expression Omnibus (GEO) databases. Data from HNSCC patients undergoing RT were extracted for analysis. TIICs prevalence in HNSCC patients was quantified by gene set variation analysis (GSVA) algorithm. TIICs and post-RT survival were analyzed using univariate Cox regression analysis and used to construct and validate a tumor-infiltrating cells score (TICS).
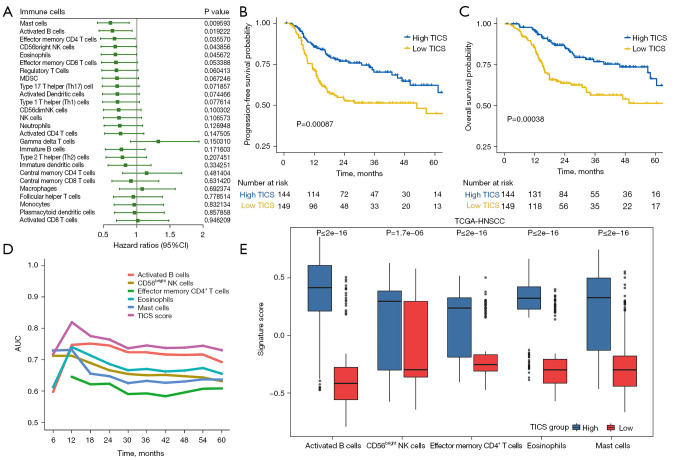
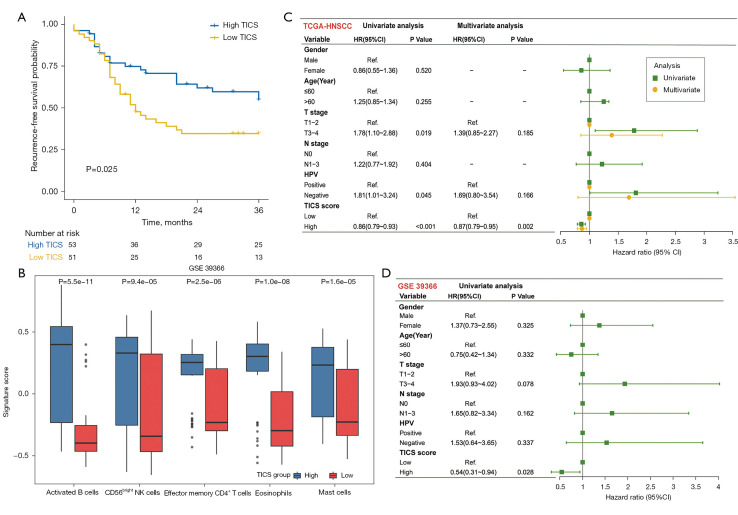
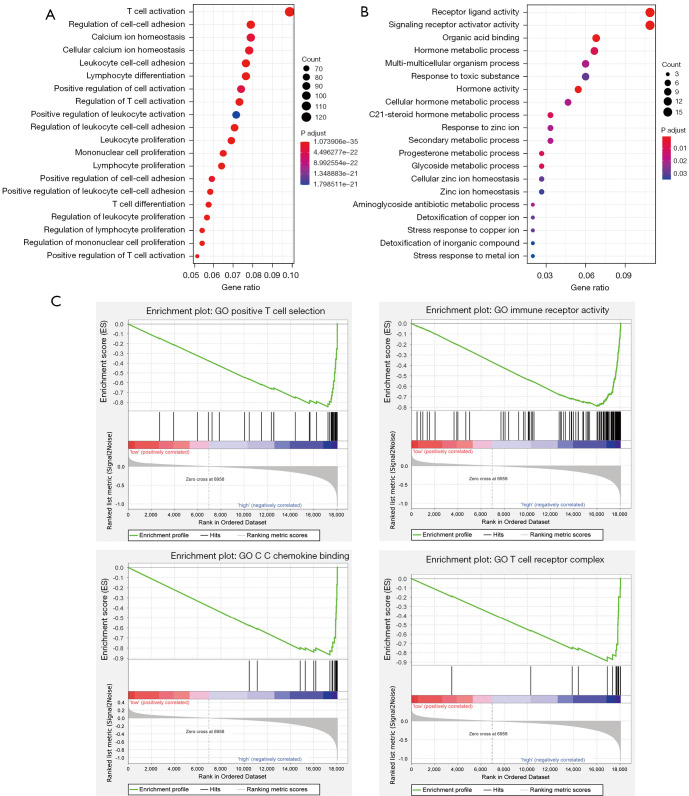
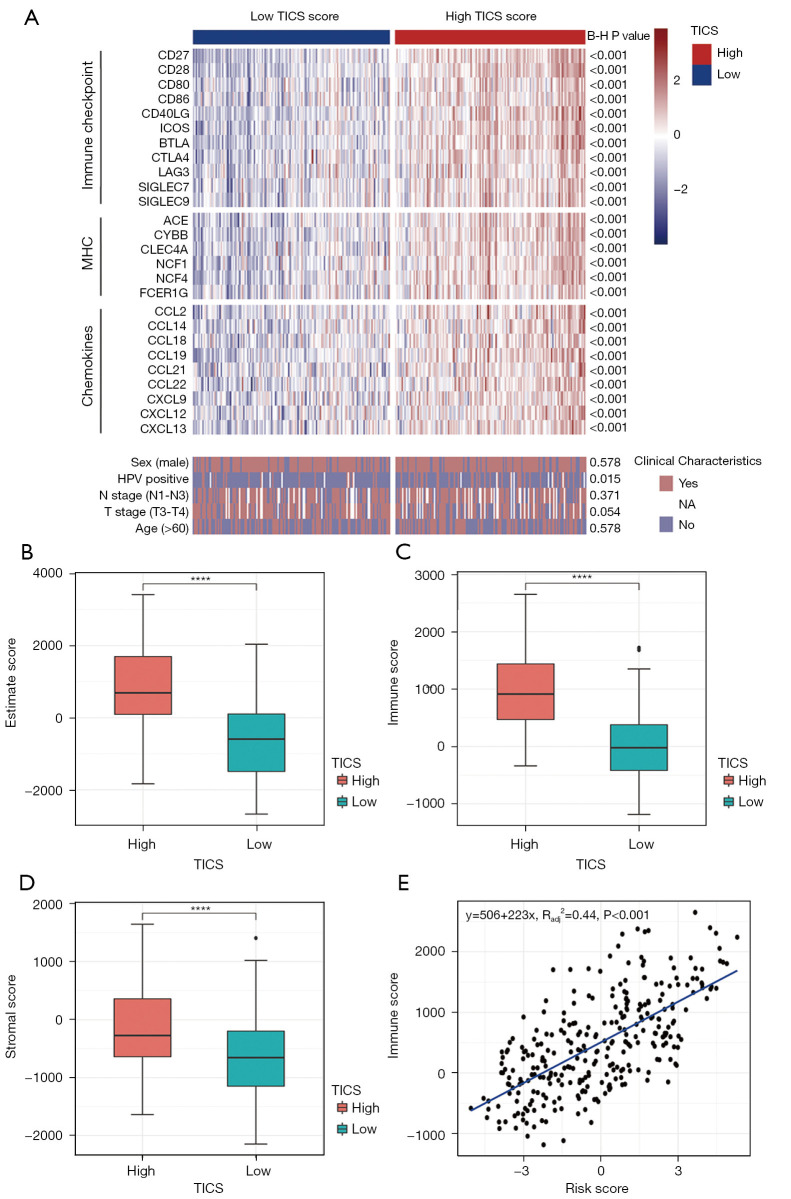
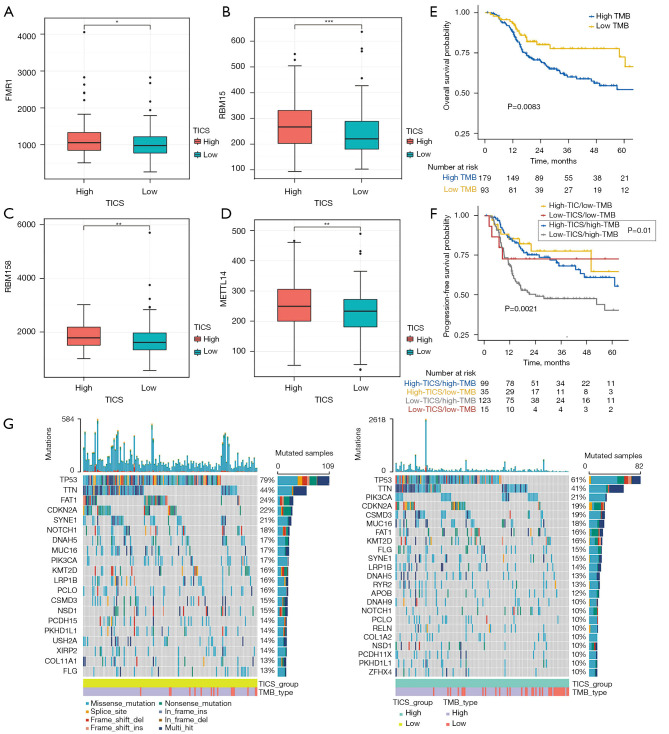
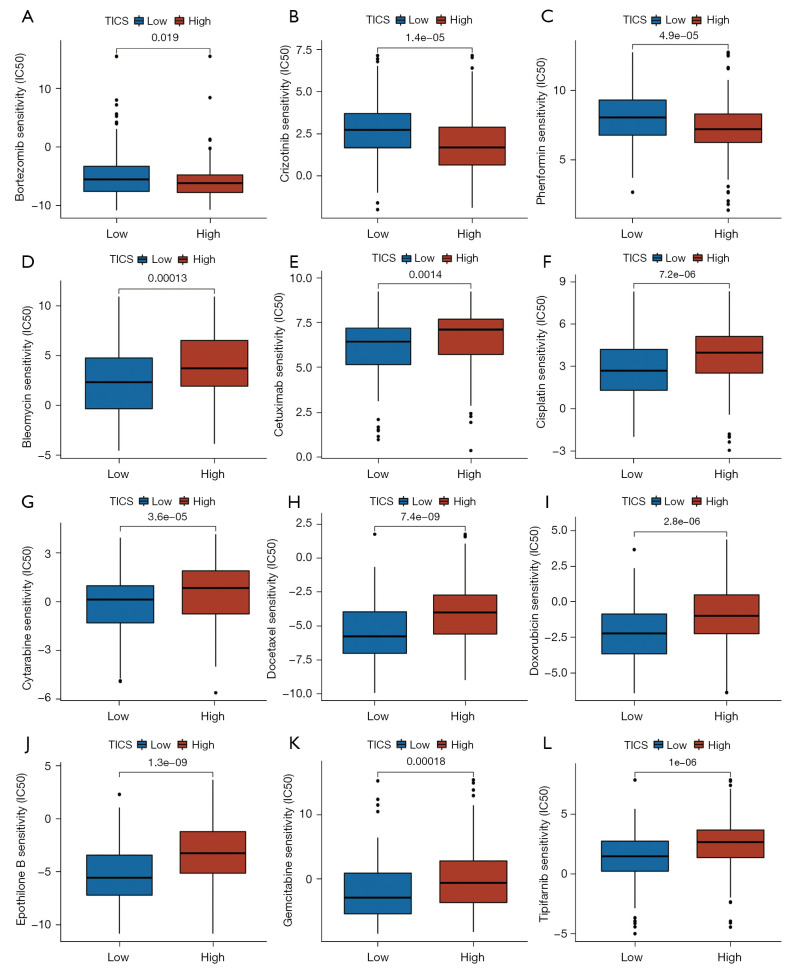
Results: Five of 26 immune cells were significantly associated with HNSCC prognosis in the training cohort (all P<0.05). Kaplan-Meier (KM) survival curves showed that patients in the high TICS group had better survival outcomes (log-rank test, P<0.05). Univariate analyses demonstrated that the TICS had independent prognostic predictive ability for RT outcomes (P<0.05). Patients with high TICS scores showed significantly higher expression of immune-related genes. Functional pathway analyses further showed that the TICS was significantly related to immune-related biological process. Stratified analyses supported integrating TICS and tumor mutation burden (TMB) into individualized treatment planning, as an adjunct to classification by clinical stage and human papillomavirus (HPV) infection.
Conclusions: The TICS model supports a personalized medicine approach to RT for HNSCC. Increased prevalence of TIIC within the tumor microenvironment (TME) confers a better prognosis for patients undergoing treatment for HNSCC.
Keywords: Head and neck squamous cell carcinoma (HNSCC); gene set variation analysis (GSVA); human papillomavirus (HPV); radiotherapy (RT); tumor-infiltrating immune cell (TIIC).
2024 Translational Cancer Research. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://tcr.amegroups.com/article/view/10.21037/tcr-23-2345/coif). The authors have no conflicts of interest to declare.
Figures

Similar articles
-
Identification and validation of a prognostic signature of autophagy, apoptosis and pyroptosis-related genes for head and neck squamous cell carcinoma: to imply therapeutic choices of HPV negative patients.Front Immunol. 2023 Jan 10;13:1100417. doi: 10.3389/fimmu.2022.1100417. eCollection 2022. Front Immunol. 2023. PMID: 36703967 Free PMC article.
-
Identification and verification of eight cancer-associated fibroblasts related genes as a prognostic signature for head and neck squamous cell carcinoma.Heliyon. 2023 Feb 28;9(3):e14003. doi: 10.1016/j.heliyon.2023.e14003. eCollection 2023 Mar. Heliyon. 2023. PMID: 36938461 Free PMC article.
-
Exploration of prognostic biomarkers in head and neck squamous cell carcinoma microenvironment from TCGA database.Ann Transl Med. 2023 Feb 28;11(4):163. doi: 10.21037/atm-22-6481. Ann Transl Med. 2023. PMID: 36923087 Free PMC article.
-
Tumor Mutation Burden, Immune Cell Infiltration, and Construction of Immune-Related Genes Prognostic Model in Head and Neck Cancer.Int J Med Sci. 2021 Jan 1;18(1):226-238. doi: 10.7150/ijms.51064. eCollection 2021. Int J Med Sci. 2021. PMID: 33390791 Free PMC article.
-
FAM3D as a Prognostic Indicator of Head and Neck Squamous Cell Carcinoma Is Associated with Immune Infiltration.Comput Math Methods Med. 2022 Dec 3;2022:5851755. doi: 10.1155/2022/5851755. eCollection 2022. Comput Math Methods Med. 2022. PMID: 36510584 Free PMC article.
Cited by
-
CCNE2 promotes cisplatin resistance and affects prognosis of head and neck squamous cell carcinoma by targeting MNAT1.Sci Rep. 2025 Apr 23;15(1):14011. doi: 10.1038/s41598-025-98989-8. Sci Rep. 2025. PMID: 40269062 Free PMC article.
References
LinkOut - more resources
Full Text Sources