

Acute kidney injury should not be neglected - optimization of quick Pitt bacteremia score for predicting mortality in critically ill patients with bloodstream infection: a retrospective cohort study
- PMID: 38410828
- PMCID: PMC10896049
- DOI: 10.1177/20499361241231147
Acute kidney injury should not be neglected - optimization of quick Pitt bacteremia score for predicting mortality in critically ill patients with bloodstream infection: a retrospective cohort study
Abstract
Background: Considering the therapeutic difficulties and mortality associated with bloodstream infection (BSI), it is essential to investigate other potential factors affecting mortality in critically ill patients with BSI and examine the utility of the quick Pitt bacteremia (qPitt) score to improve the survival rate.
Objectives: To improve the predictive accuracy of the qPitt scoring system by evaluating the five current components of qPitt and including other potential factors influencing mortality in critically ill patients with BSI.
Design: This was a retrospective cohort study.
Methods: Medical information from the Medical Information Mart for Intensive Care IV database was used in this retrospective cohort study. The risk factors associated with mortality were examined using a multivariate logistic regression model. The area under the receiver operating characteristic curve (AUC) was used to assess the discriminatory capability of the prediction models.
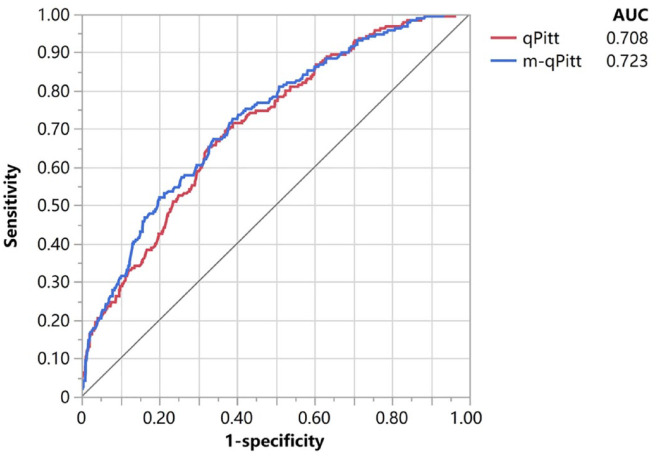
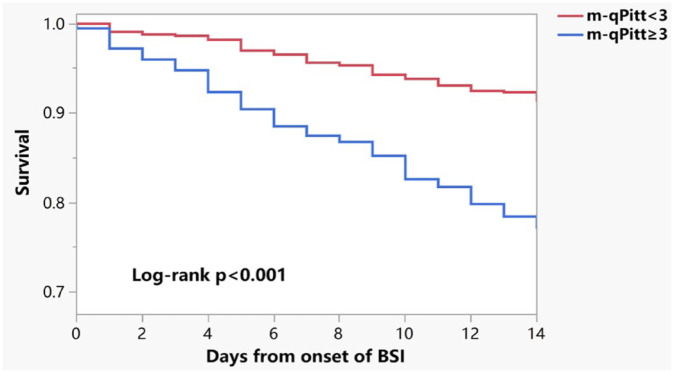
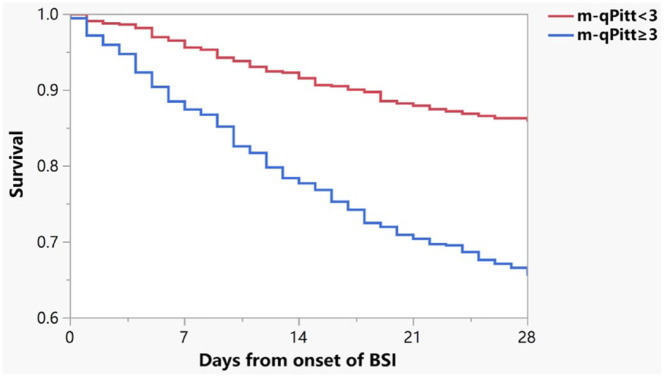
Results: In total, 1240 eligible critically ill patients with BSI were included. After adjustment for age, community-onset BSI, indwelling invasive lines, and Glasgow Coma Scale (GCS) ⩽ 8, acute kidney injury (AKI) was identified as a notable risk factor for 14-day mortality. Except for altered mental status, the four other main components of the original qPitt were significantly associated with 14-day mortality. Hence, we established a modified qPitt (m-qPitt) by adding AKI and replacing altered mental status with GCS ⩽ 8. The AUCs for m-qPitt and qPitt were 0.723 [95% confidence interval (CI): 0.683-0.759] and 0.708 (95% CI: 0.669-0.745) in predicting 14-day mortality, respectively. Moreover, m-qPitt also had acceptable performance and discrimination power [0.700 (95% CI: 0.666-0.732)] in predicting 28-day mortality.
Conclusion: AKI significantly influenced the survival of critically ill patients with BSIs. Compared with the original qPitt, our new m-qPitt was proven to have a better predictive performance for mortality in critically ill patients with BSI. Further studies should be conducted to validate the practicality of m-qPitt.
Keywords: Glasgow Coma Scale; acute kidney injury; bloodstream infection; mortality; quick Pitt bacteremia score.
© The Author(s), 2024.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Figures


References
-
- Vallés J, Ferrer R. Bloodstream infection in the ICU. Infect Dis Clin North Am 2009; 23: 557–569. - PubMed
-
- Bone RC, Balk RA, Cerra FB, et al. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Chest 1992; 101: 1644–1655. - PubMed
-
- Battle SE, Augustine MR, Watson CM, et al. Derivation of a quick Pitt bacteremia score to predict mortality in patients with Gram-negative bloodstream infection. Infection 2019; 47: 571–578. - PubMed
LinkOut - more resources
Full Text Sources
