

Sex Differences in Revascularization, Treatment Goals, and Outcomes of Patients With Chronic Coronary Disease: Insights From the ISCHEMIA Trial
- PMID: 38410945
- PMCID: PMC10944079
- DOI: 10.1161/JAHA.122.029850
Sex Differences in Revascularization, Treatment Goals, and Outcomes of Patients With Chronic Coronary Disease: Insights From the ISCHEMIA Trial
Abstract
Background: Women with chronic coronary disease are generally older than men and have more comorbidities but less atherosclerosis. We explored sex differences in revascularization, guideline-directed medical therapy, and outcomes among patients with chronic coronary disease with ischemia on stress testing, with and without invasive management.
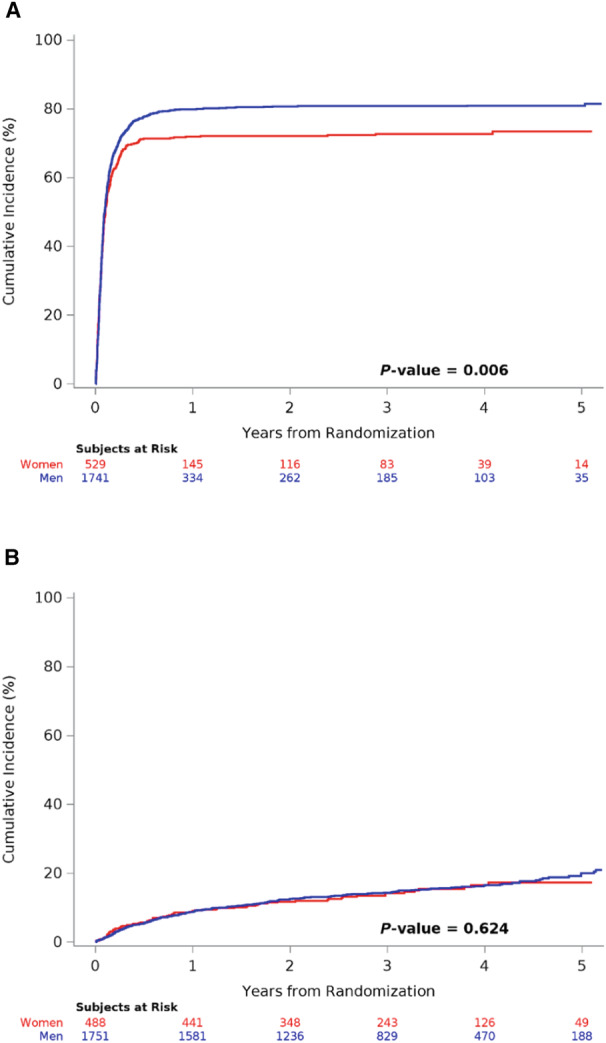
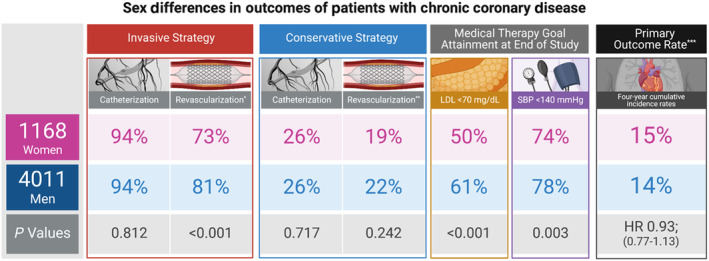
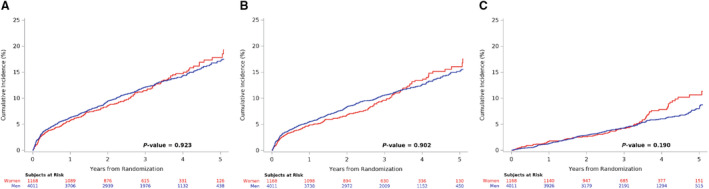
Methods and results: The ISCHEMIA (International Study of Comparative Health Effectiveness with Medical and Invasive Approaches) trial randomized patients with moderate or severe ischemia to invasive management with angiography, revascularization, and guideline-directed medical therapy, or initial conservative management with guideline-directed medical therapy alone. We evaluated the primary outcome (cardiovascular death, myocardial infarction, or hospitalization for unstable angina, heart failure, or resuscitated cardiac arrest) and other end points, by sex, in 1168 (22.6%) women and 4011 (77.4%) men. Invasive group catheterization rates were similar, with less revascularization among women (73.4% of invasive-assigned women revascularized versus 81.2% of invasive-assigned men; P<0.001). Women had less coronary artery disease: multivessel in 60.0% of invasive-assigned women and 74.8% of invasive-assigned men, and no ≥50% stenosis in 12.3% versus 4.5% (P<0.001). In the conservative group, 4-year catheterization rates were 26.3% of women versus 25.6% of men (P=0.72). Guideline-directed medical therapy use was lower among women with fewer risk factor goals attained. There were no sex differences in the primary outcome (adjusted hazard ratio [HR] for women versus men, 0.93 [95% CI, 0.77-1.13]; P=0.47) or the major secondary outcome of cardiovascular death/myocardial infarction (adjusted HR, 0.93 [95% CI, 0.76-1.14]; P=0.49), with no significant sex-by-treatment-group interactions.
Conclusions: Women had less extensive coronary artery disease and, therefore, lower revascularization rates in the invasive group. Despite lower risk factor goal attainment, women with chronic coronary disease experienced similar risk-adjusted outcomes to men in the ISCHEMIA trial.
Registration: URL: http://wwwclinicaltrials.gov. Unique identifier: NCT01471522.
Keywords: coronary artery disease; ischemic heart disease; sex differences; women's health.
Figures
References
-
- Jespersen L, Hvelplund A, Abildstrøm SZ, Pedersen F, Galatius S, Madsen JK, Jørgensen E, Kelbæk H, Prescott E. Stable angina pectoris with no obstructive coronary artery disease is associated with increased risks of major adverse cardiovascular events. Eur Heart J. 2012;33:734–744. doi: 10.1093/eurheartj/ehr331 - DOI - PubMed
-
- Sharaf B, Wood T, Shaw L, Johnson BD, Kelsey S, Anderson RD, Pepine CJ, Merz CN. Adverse outcomes among women presenting with signs and symptoms of ischemia and no obstructive coronary artery disease: findings from the National Heart, Lung, and Blood Institute‐sponsored Women's ischemia syndrome evaluation (WISE) angiographic core laboratory. Am Heart J. 2013;166:134–141. doi: 10.1016/j.ahj.2013.04.002 - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
