

Fleischner Society: Glossary of Terms for Thoracic Imaging
- PMID: 38411514
- PMCID: PMC10902601
- DOI: 10.1148/radiol.232558
Fleischner Society: Glossary of Terms for Thoracic Imaging
Abstract
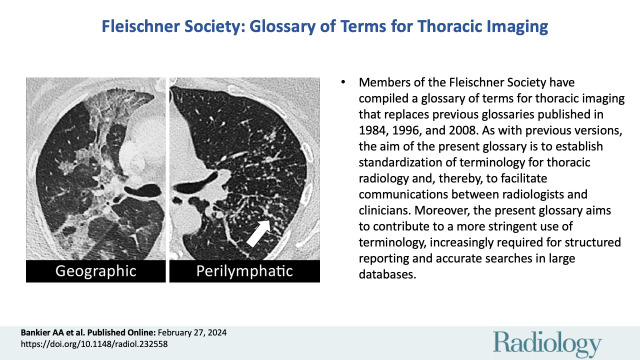
Members of the Fleischner Society have compiled a glossary of terms for thoracic imaging that replaces previous glossaries published in 1984, 1996, and 2008, respectively. The impetus to update the previous version arose from multiple considerations. These include an awareness that new terms and concepts have emerged, others have become obsolete, and the usage of some terms has either changed or become inconsistent to a degree that warranted a new definition. This latest glossary is focused on terms of clinical importance and on those whose meaning may be perceived as vague or ambiguous. As with previous versions, the aim of the present glossary is to establish standardization of terminology for thoracic radiology and, thereby, to facilitate communications between radiologists and clinicians. Moreover, the present glossary aims to contribute to a more stringent use of terminology, increasingly required for structured reporting and accurate searches in large databases. Compared with the previous version, the number of images (chest radiography and CT) in the current version has substantially increased. The authors hope that this will enhance its educational and practical value. All definitions and images are hyperlinked throughout the text. Click on each figure callout to view corresponding image. © RSNA, 2024 Supplemental material is available for this article. See also the editorials by Bhalla and Powell in this issue.
Conflict of interest statement
Figures





























Comment in
-
Fleischner Society Glossary: The Power of Standardization of Nomenclature for Thoracic Surgical Communications.Radiology. 2024 Mar;310(3):e240410. doi: 10.1148/radiol.240410. Radiology. 2024. PMID: 38530187 No abstract available.
-
Speaking the Same Language: The Fleischner Society Glossary for Thoracic Imaging.Radiology. 2024 Mar;310(3):e240414. doi: 10.1148/radiol.240414. Radiology. 2024. PMID: 38530190 Free PMC article. No abstract available.
-
Glossary of Terms for Thoracic Imaging: Implications for Machine Learning and Future Practice.Radiology. 2024 Jun;311(3):e240907. doi: 10.1148/radiol.240907. Radiology. 2024. PMID: 38832883 No abstract available.
-
Diffuse Parenchymal Lung Disease and the Inherent Limitations of a Glossary.Radiology. 2024 Jun;311(3):e240948. doi: 10.1148/radiol.240948. Radiology. 2024. PMID: 38832884 No abstract available.
References
-
- Tuddenham WJ . Glossary of terms for thoracic radiology: recommendations of the Nomenclature Committee of the Fleischner Society . AJR Am J Roentgenol 1984. ; 143 ( 3 ): 509 – 517 . - PubMed
-
- Austin JH , Müller NL , Friedman PJ , et al. . Glossary of terms for CT of the lungs: recommendations of the Nomenclature Committee of the Fleischner Society . Radiology 1996. ; 200 ( 2 ): 327 – 331 . - PubMed
-
- Hansell DM , Bankier AA , MacMahon H , McLoud TC , Müller NL , Remy J . Fleischner Society: glossary of terms for thoracic imaging . Radiology 2008. ; 246 ( 3 ): 697 – 722 . - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
