

Rotator cuff tear patterns: MRI appearance and its surgical relevance
- PMID: 38411840
- PMCID: PMC10899560
- DOI: 10.1186/s13244-024-01607-w
Rotator cuff tear patterns: MRI appearance and its surgical relevance
Abstract
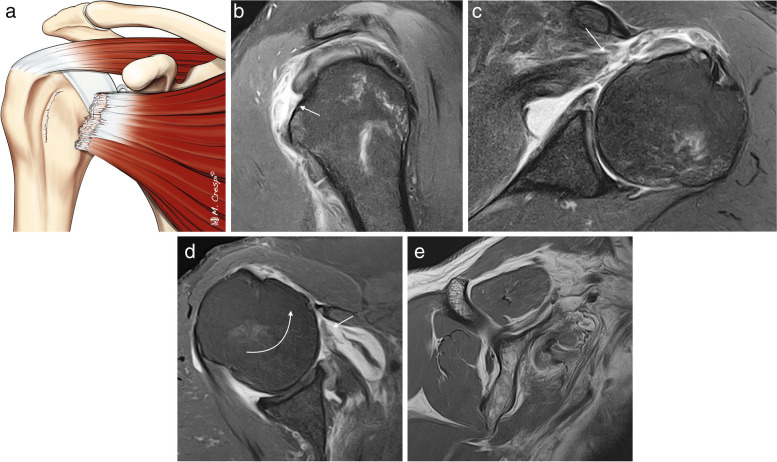
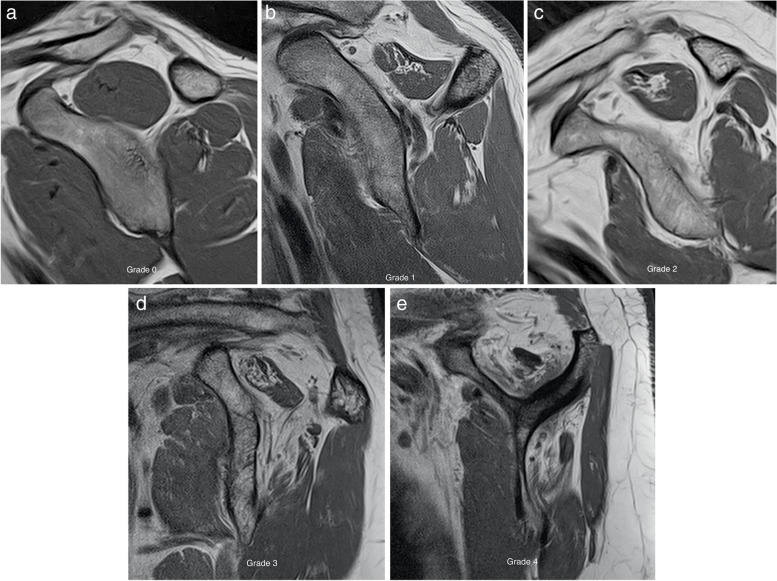
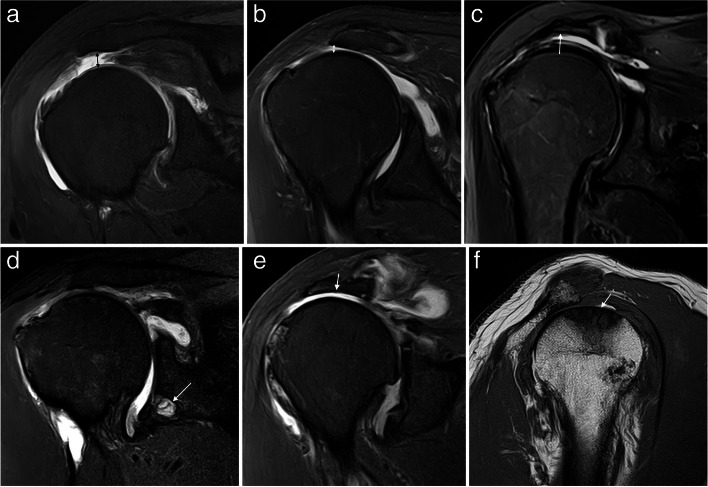
A new perspective on rotator cuff anatomy has allowed a better understanding of the patterns of the different rotator cuff tears. It is essential for radiologists to be aware of these different patterns of tears and to understand how they might influence treatment and surgical approach. Our objective is to review the arthroscopy correlated magnetic resonance imaging appearance of the different types of rotator cuff tears based on current anatomical concepts.Critical relevance statement Knowledge of the characteristics of rotator cuff tears improves our communication with the surgeon and can also make it easier for the radiologist to prepare a report that guides therapeutic conduct and serves as a prognosis for the patient.Key points• There is no universally accepted classification for RC tears.• New patterns such as delamination or myotendinous junction tears have been defined.• The most difficult feature to assess in full thickness tears on MRI is the pattern.• Fatty infiltration of the RC tendons is crucial in the prognosis and outcome.• The radiological report is an effective way of communication with the surgeon.
Keywords: Delaminated; Massive tears; Outcome; Rotator cuff; Surgery.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

















References
-
- Calvo E, Rebollon GC, Morcillo D, Arce G. Rotator Cuff Across the Life Span ISAKOS Consensus Book. New York: Springer; 2019. Diagnosis and Classification of Rotator Cuff Tears.
-
- Oñate M, Bureau NJ (2019) Supraspinatus myotendinous junction injuries: MRI Findings and prevalence. AJR Am J Roentgenol 212(1):W1–W9 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
