

Liver imaging and pregnancy: what to expect when your patient is expecting
- PMID: 38411871
- PMCID: PMC10899155
- DOI: 10.1186/s13244-024-01622-x
Liver imaging and pregnancy: what to expect when your patient is expecting
Abstract
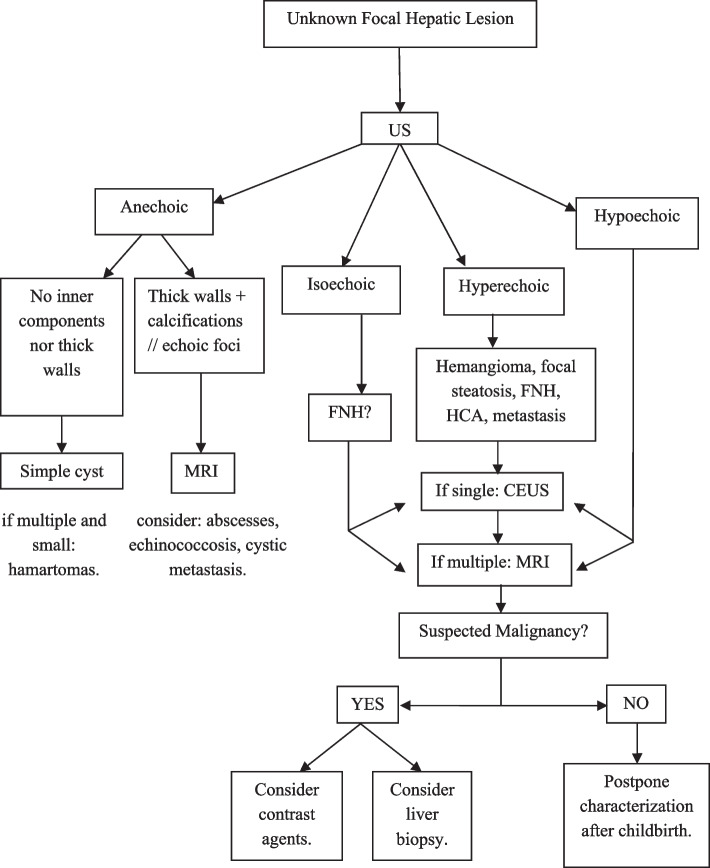
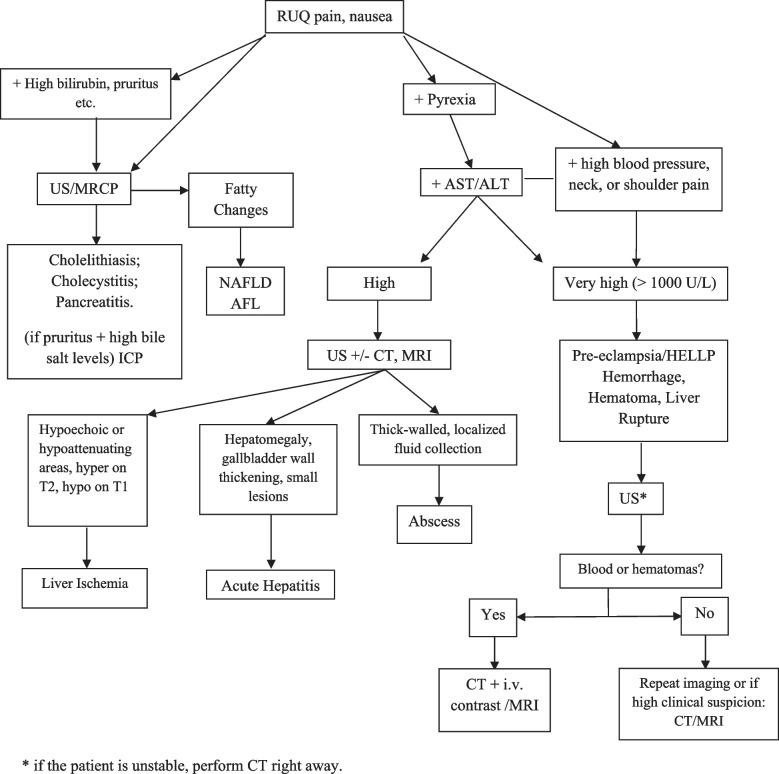
Liver diseases in pregnancy can be specific to gestation or only coincidental. In the latter case, the diagnosis can be difficult. Rapid diagnosis of maternal-fetal emergencies and situations requiring specialized interventions are crucial to preserve the maternal liver and guarantee materno-fetal survival. While detailed questioning of the patient and a clinical examination are highly important, imaging is often essential to reach a diagnosis of these liver diseases and lesions. Three groups of liver diseases may be observed during pregnancy: (1) diseases related to pregnancy: intrahepatic cholestasis of pregnancy, pre-eclampsia, eclampsia, hemolysis, elevated liver enzymes and low platelets (HELLP) syndrome, and acute fatty liver of pregnancy; (2) liver diseases that are more frequent during or exacerbated by pregnancy: acute herpes simplex hepatitis, Budd-Chiari syndrome, hemorrhagic hereditary telangiectasia, hepatocellular adenoma, portal vein thrombosis, and cholelithiasis; (3) coincidental conditions, including acute hepatitis, incidental focal liver lesions, metabolic dysfunction-associated steatotic liver disease, cirrhosis, hepatocellular carcinoma, liver abscesses and parasitosis, and liver transplantation. Specific knowledge of the main imaging findings is required to reach an early diagnosis, for adequate follow-up, and to avoid adverse consequences in both the mother and the fetus.Critical relevance statement Pregnancy-related liver diseases are the most important cause of liver dysfunction in pregnant patients and, in pregnancy, even common liver conditions can have an unexpected turn. Fear of radiations should never delay necessary imaging studies in pregnancy.Key points• Pregnancy-related liver diseases are the most frequent cause of liver dysfunction during gestation.• Fear of radiation should never delay necessary imaging studies.• Liver imaging is important to assess liver emergencies and for the diagnosis and follow-up of any other liver diseases.• Common liver conditions and lesions may take an unexpected turn during pregnancy.• Pregnancy-specific diseases such as pre-eclampsia and HELLP syndrome must be rapidly identified. However, imaging should never delay delivery when it is considered to be urgent for maternal-fetal survival.
Keywords: Complications; Focal liver lesions; Liver disorders; Liver transplant; Pregnancy.
© 2024. The Author(s).
Conflict of interest statement
GP, JB, A.A., G.B., MDB, and VV declare that they have nothing to disclose. RC is a member of the
Figures
Similar articles
-
Liver pathology in pregnancy.Pathol Int. 2022 Jan;72(1):1-13. doi: 10.1111/pin.13186. Epub 2021 Nov 24. Pathol Int. 2022. PMID: 34818440 Review.
-
Liver disease in pregnancy: Medical aspects and their implications for mother and child.Ann Hepatol. 2019 Jul-Aug;18(4):553-562. doi: 10.1016/j.aohep.2019.04.009. Epub 2019 May 6. Ann Hepatol. 2019. PMID: 31126882 Review.
-
Liver disease in pregnancy.Hepatology. 2008 Mar;47(3):1067-76. doi: 10.1002/hep.22130. Hepatology. 2008. PMID: 18265410 Review.
-
State of the Art in Hepatic Dysfunction in Pregnancy.Healthcare (Basel). 2021 Oct 31;9(11):1481. doi: 10.3390/healthcare9111481. Healthcare (Basel). 2021. PMID: 34828527 Free PMC article. Review.
-
Hepatic disorders severely affected by pregnancy: medical and obstetric management.Med Clin North Am. 2008 Jul;92(4):739-60, vii-viii. doi: 10.1016/j.mcna.2008.03.002. Med Clin North Am. 2008. PMID: 18570941 Review.
Cited by
-
Differentially expressed genes in the placentas with pre-eclampsia and fetal growth restriction using RNA sequencing and verification.J Perinat Med. 2025 Apr 28;53(5):595-603. doi: 10.1515/jpm-2025-0025. Print 2025 Jun 26. J Perinat Med. 2025. PMID: 40285515
-
Development and psychometric evaluation of the fear of medical imaging radiation scale (FOMIRS): insights from multimethod analysis.Insights Imaging. 2025 Jun 27;16(1):140. doi: 10.1186/s13244-025-02018-1. Insights Imaging. 2025. PMID: 40579622 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
