

Tumor-Stroma Proportion to Predict Chemoresistance in Patients With Ovarian Cancer
- PMID: 38411963
- PMCID: PMC10900967
- DOI: 10.1001/jamanetworkopen.2024.0407
Tumor-Stroma Proportion to Predict Chemoresistance in Patients With Ovarian Cancer
Abstract
Importance: Platinum-based chemotherapy is the backbone of standard-of-care treatment for patients with advanced-stage, high-grade serous carcinoma (HGSC), the most common form of ovarian cancer; however, one-third of patients have or acquire chemoresistance toward platinum-based therapies.
Objective: To demonstrate the utility of tumor-stroma proportion (TSP) as a predictive biomarker of chemoresistance of HGSC, progression-free survival (PFS), and overall survival (OS).
Design, setting, and participants: This prognostic study leveraged tumors from patients with HGSC in The Cancer Genome Atlas (TCGA) cohort (1993-2013) and an independent cohort of resected clinical specimens from patients with HGSC (2004-2014) available in diagnostic and tissue microarray formats from the University of Tübingen in Germany. Data analysis was conducted from January 2021 to January 2024.
Exposure: Diagnosis of HGSC.
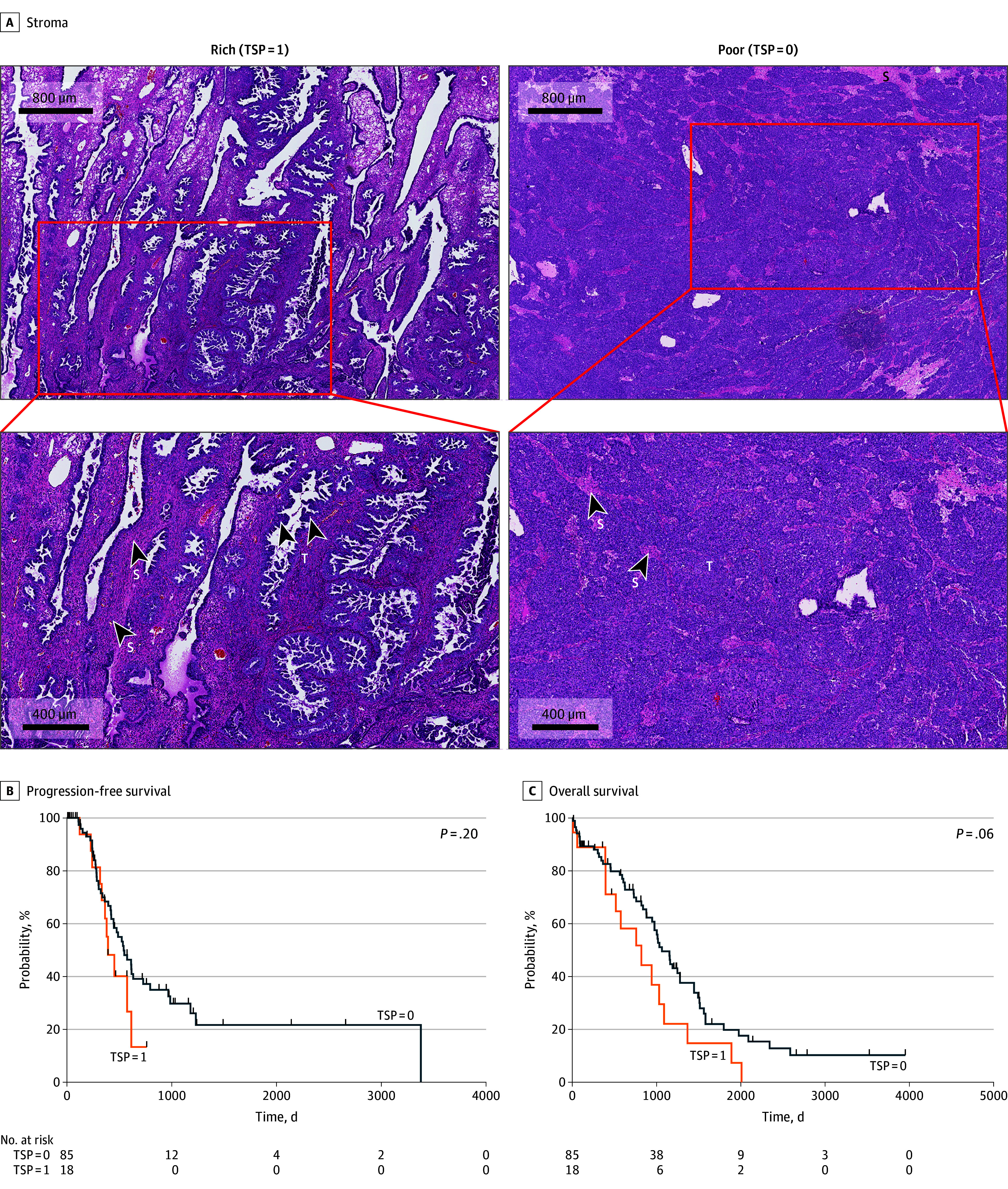
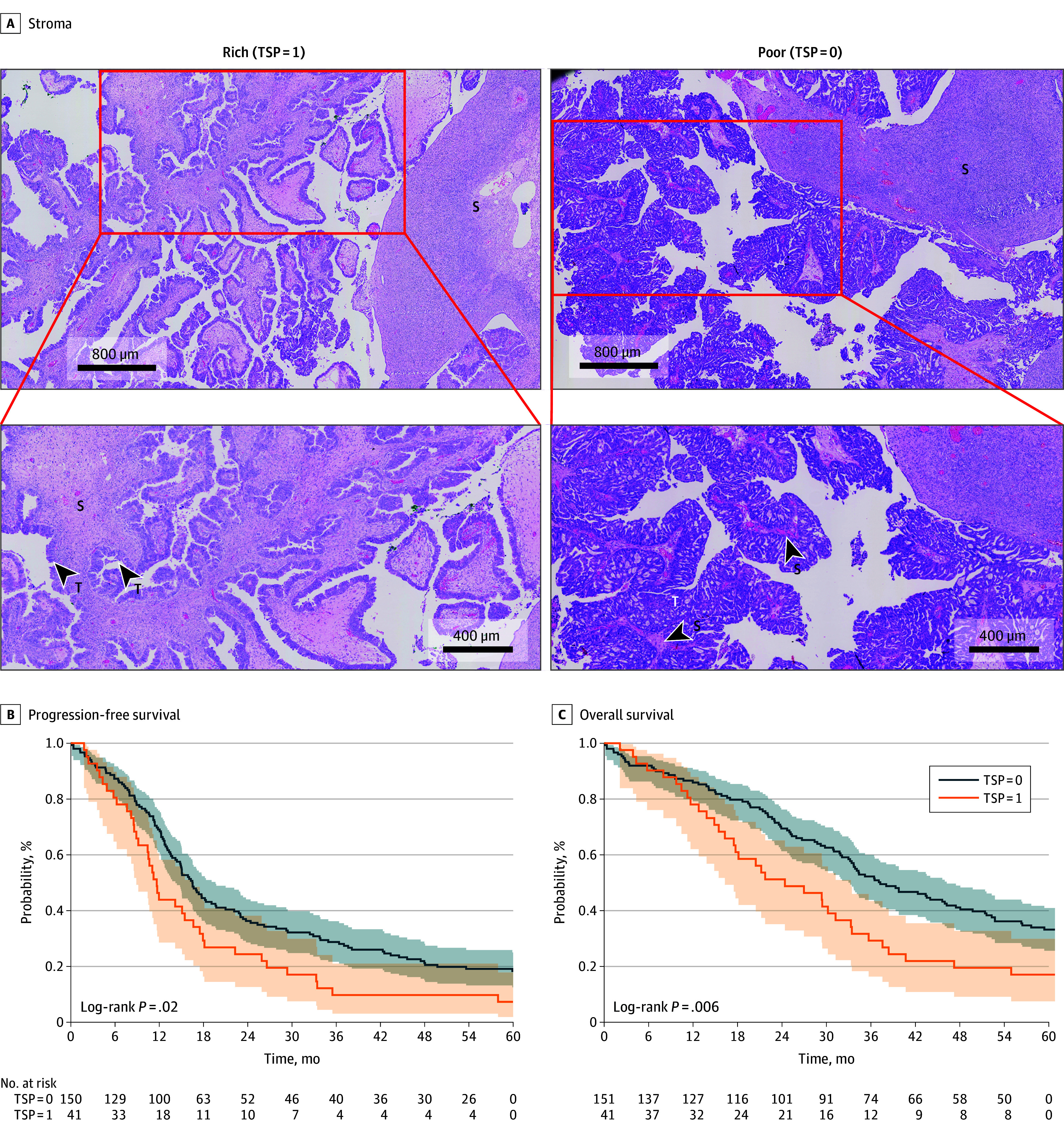
Main outcomes and measures: Principal outcome measures were the ability of TSP to predict platinum chemoresistance, PFS, and OS. Using hematoxylin and eosin-stained slides from the Tübingen cohort (used for routine diagnostic assessment from surgical specimens) as well as tissue microarrays, representative sections of tumors for scoring of TSP were identified using previously evaluated cutoffs of 50% stroma or greater (high TSP) and less than 50% stroma (low TSP). Digitized slides from the TCGA Cohort were analyzed and scored in a similar fashion. Kaplan-Meier time-to-event functions were fit to estimate PFS and OS.
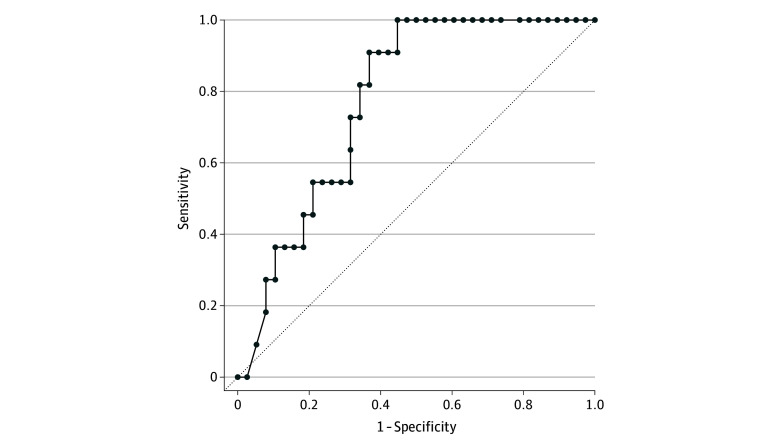
Results: The study included 103 patients (mean [SD] age, 61.6 [11.1] years) from the TCGA cohort and 192 patients (mean [SD] age at diagnosis, 63.7 [11.1] years) from the Tübingen cohort. In the TCGA cohort, there was no significant association of TSP levels with chemoresistance, PFS, or OS. However, in the Tübingen cohort, high TSP was associated with significantly shorter PFS (HR, 1.586; 95% CI, 1.093-2.302; P = .02) and OS (hazard ratio [HR], 1.867; 1.249-2.789; P = .002). Patients with chemoresistant tumors were twice as likely to have high TSP as compared to patients with chemosensitive tumors (HR, 2.861; 95% CI, 1.256-6.515; P = .01). In tissue microarrays from 185 patients from the Tübingen cohort, high TSP was again associated with significantly shorter PFS (HR, 1.675; 95% CI, 1.012-2.772 P = .04) and OS (HR, 2.491; 95% CI, 1.585-3.912; P < .001).
Conclusions and relevance: In this prognostic study, TSP was a consistent and reproducible marker of clinical outcome measures of HGSC, including PFS, OS, and platinum chemoresistance. Accurate and cost-effective predictive biomarkers of platinum chemotherapy resistance are needed to identify patients most likely to benefit from standard treatments, and TSP can easily be implemented and integrated into prospective clinical trial design and adapted to identify patients who are least likely to benefit long-term from conventional platinum-based cytotoxic chemotherapy treatment at the time of initial diagnosis.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
