

Rapid genomic sequencing for genetic disease diagnosis and therapy in intensive care units: a review
- PMID: 38413639
- PMCID: PMC10899612
- DOI: 10.1038/s41525-024-00404-0
Rapid genomic sequencing for genetic disease diagnosis and therapy in intensive care units: a review
Abstract
Single locus (Mendelian) diseases are a leading cause of childhood hospitalization, intensive care unit (ICU) admission, mortality, and healthcare cost. Rapid genome sequencing (RGS), ultra-rapid genome sequencing (URGS), and rapid exome sequencing (RES) are diagnostic tests for genetic diseases for ICU patients. In 44 studies of children in ICUs with diseases of unknown etiology, 37% received a genetic diagnosis, 26% had consequent changes in management, and net healthcare costs were reduced by $14,265 per child tested by URGS, RGS, or RES. URGS outperformed RGS and RES with faster time to diagnosis, and higher rate of diagnosis and clinical utility. Diagnostic and clinical outcomes will improve as methods evolve, costs decrease, and testing is implemented within precision medicine delivery systems attuned to ICU needs. URGS, RGS, and RES are currently performed in <5% of the ~200,000 children likely to benefit annually due to lack of payor coverage, inadequate reimbursement, hospital policies, hospitalist unfamiliarity, under-recognition of possible genetic diseases, and current formatting as tests rather than as a rapid precision medicine delivery system. The gap between actual and optimal outcomes in children in ICUs is currently increasing since expanded use of URGS, RGS, and RES lags growth in those likely to benefit through new therapies. There is sufficient evidence to conclude that URGS, RGS, or RES should be considered in all children with diseases of uncertain etiology at ICU admission. Minimally, diagnostic URGS, RGS, or RES should be ordered early during admissions of critically ill infants and children with suspected genetic diseases.
© 2024. The Author(s).
Conflict of interest statement
RN and KE report there are no competing interests to declare. SFK is an editor of npj Genomic Medicine.
Figures
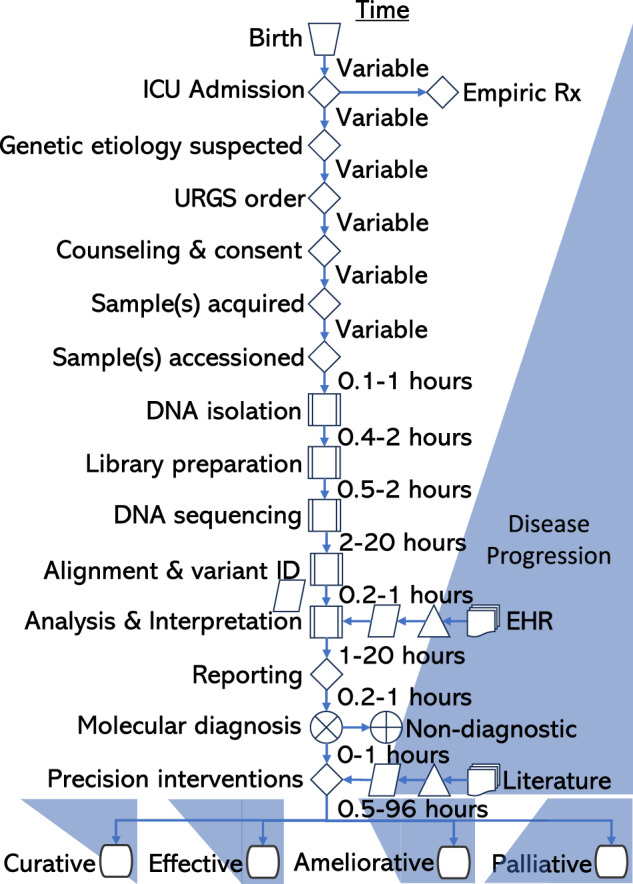
 manual operation;
manual operation;  decision;
decision;  predefined process;
predefined process;  data;
data;  extract;
extract;  multidocument;
multidocument;  summing junction;
summing junction; or;
or;  terminator.
terminator.
References
-
- The Holy Bible, New International Version, HarperCollins, 1973/2011, Isaiah 65.
-
- Ely DM, Driscoll AK. Infant mortality in the United States: Provisional data from the 2022 period linked birth/infant death file. National Center for Health Statistics. Vital Statistics Rapid Release; no 33. Hyattsville, MD: National Center for Health Statistics. 10.15620/cdc:133699 (2023).
-
- OECD. Health at a Glance 2023: OECD Indicators, OECD Publishing, Paris, 10.1787/7a7afb35-en (2023).
-
- Verma IC, Puri RD. Global burden of genetic disease and the role of genetic screening. Semin. Fetal Neonatal Med. 2015;20:354–363. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
