

Cross-country analysis of contextual factors and implementation strategies in under-5 mortality reduction in six low- and middle-income countries 2000-2015
- PMID: 38413879
- PMCID: PMC10900537
- DOI: 10.1186/s12887-023-03906-5
Cross-country analysis of contextual factors and implementation strategies in under-5 mortality reduction in six low- and middle-income countries 2000-2015
Abstract
Background: The Exemplars in Under-5 Mortality (U5M) was a multiple cases study of how six low- and middle-income countries (LMICs), Bangladesh, Ethiopia, Nepal, Peru, Rwanda, and Senegal, implemented health system-delivered evidence-based interventions (EBIs) to reduce U5M between 2000 and 2015 more effectively than others in their regions or with similar economic growth. Using implementation research, we conducted a cross-country analysis to compare decision-making pathways for how these countries chose, implemented, and adapted strategies for health system-delivered EBIs that mitigated or leveraged contextual factors to improve implementation outcomes in reducing amenable U5M.
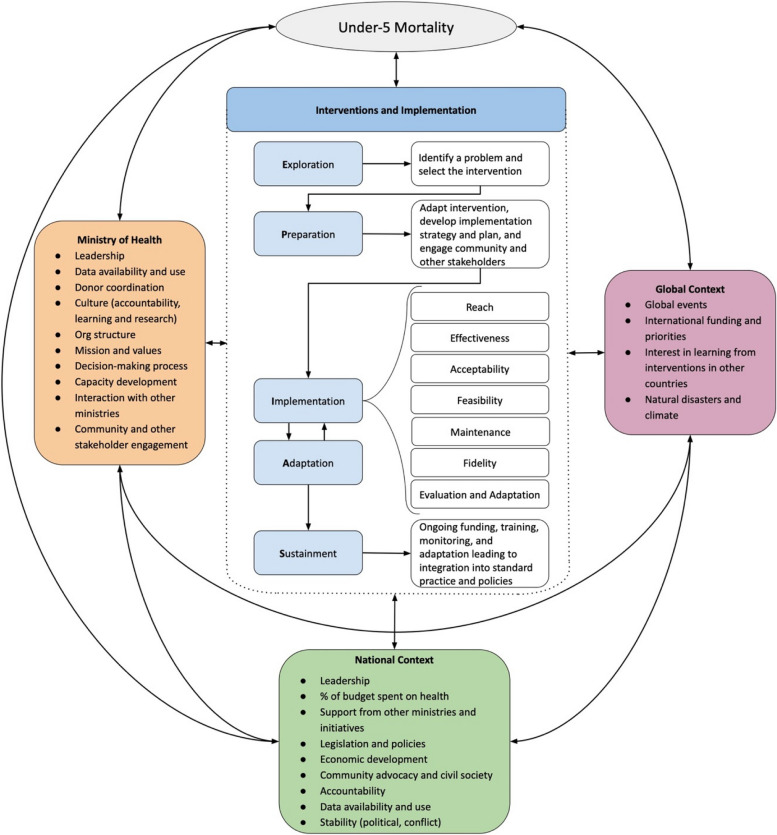
Methods: The cross-country analysis was based on the hybrid mixed methods implementation research framework used to inform the country case studies. The framework included a common pathway of Exploration, Preparation, Implementation, Adaptation, and Sustainment (EPIAS). From the existing case studies, we extracted contextual factors which were barriers, facilitators, or determinants of strategic decisions; strategies to implement EBIs; and implementation outcomes including acceptability and coverage. We identified common factors and strategies shared by countries, and individual approaches used by countries reflecting differences in contextual factors and goals.
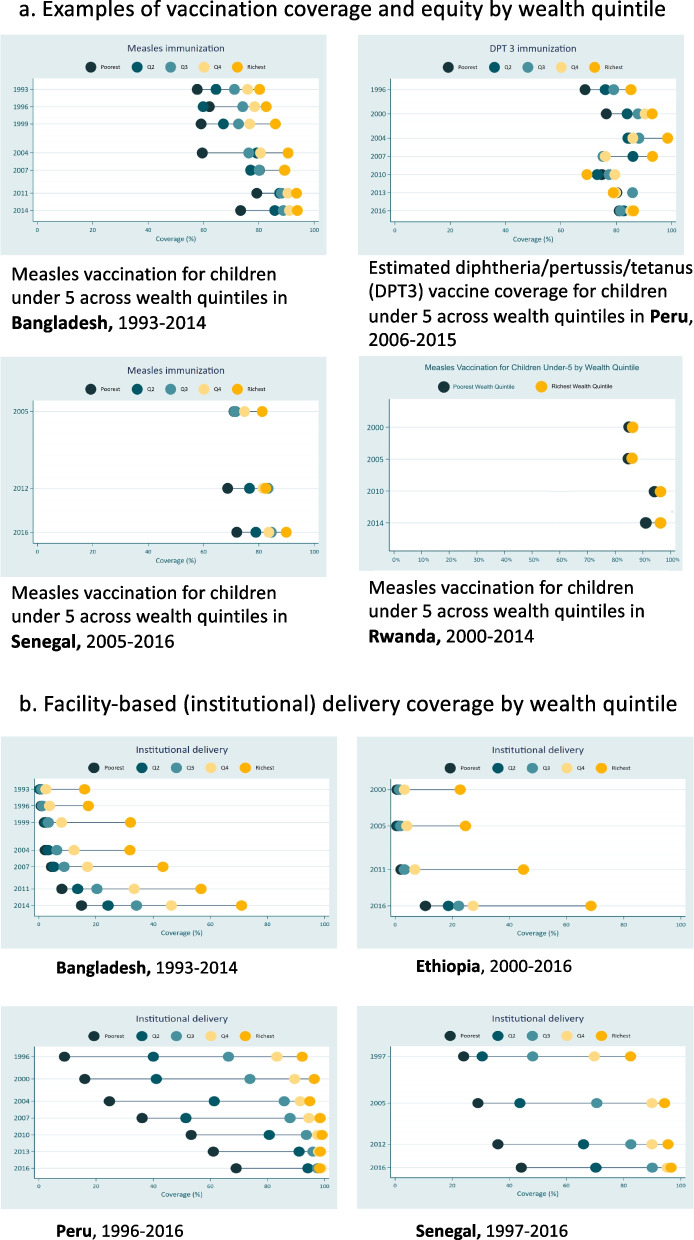
Results: We found the six countries implemented many of the same EBIs, often using similar strategies with adaptations to local context and disease burden. Common implementation strategies included use of data by decision-makers to identify problems and prioritize EBIs, determine implementation strategies and their adaptation, and measure outcomes; leveraging existing primary healthcare systems; and community and stakeholder engagement. We also found common facilitators included culture of donor and partner coordination and culture and capacity of data use, while common barriers included geography and culture and beliefs. We found evidence for achieving implementation outcomes in many countries and EBIs including acceptability, coverage, equity, and sustainability.
Discussion: We found all six countries used a common pathway to implementation with a number of strategies common across EBIs and countries which contributed to progress, either despite contextual barriers or by leveraging facilitators. The transferable knowledge from this cross-country study can be used by other countries to more effectively implement EBIs known to reduce amenable U5M and contribute to strengthening health system delivery now and in the future.
Keywords: Amenable mortality; Contextual factors; Evidence-based interventions; Implementation research; Implementation strategies; Low- and middle-income countries; Under-5 mortality.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Ruhago GM, Ngalesoni FN, Norheim OF. Addressing inequity to achieve the maternal and child health millennium development goals: looking beyond averages. BMC Public Health. 2012;12(1) Available from: https://pubmed.ncbi.nlm.nih.gov/23270489/. Cited 2021 Mar 14. - PMC - PubMed
-
- UNICEF DATA. Under-five Mortality. unicef. 2020. Available from: https://data.unicef.org/topic/child-survival/under-five-mortality/. Cited 2021 Feb 25.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
