

Mesenchymal stromal cells plus basiliximab improve the response of steroid-refractory acute graft-versus-host disease as a second-line therapy: a multicentre, randomized, controlled trial
- PMID: 38413930
- PMCID: PMC10900595
- DOI: 10.1186/s12916-024-03275-5
Mesenchymal stromal cells plus basiliximab improve the response of steroid-refractory acute graft-versus-host disease as a second-line therapy: a multicentre, randomized, controlled trial
Abstract
Background: For patients with steroid-refractory acute graft-versus-host disease (SR-aGVHD), effective second-line regimens are urgently needed. Mesenchymal stromal cells (MSCs) have been used as salvage regimens for SR-aGVHD in the past. However, clinical trials and an overall understanding of the molecular mechanisms of MSCs combined with basiliximab for SR-aGVHD are limited, especially in haploidentical haemopoietic stem cell transplantation (HID HSCT).
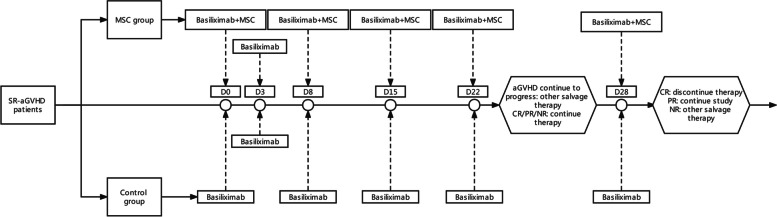
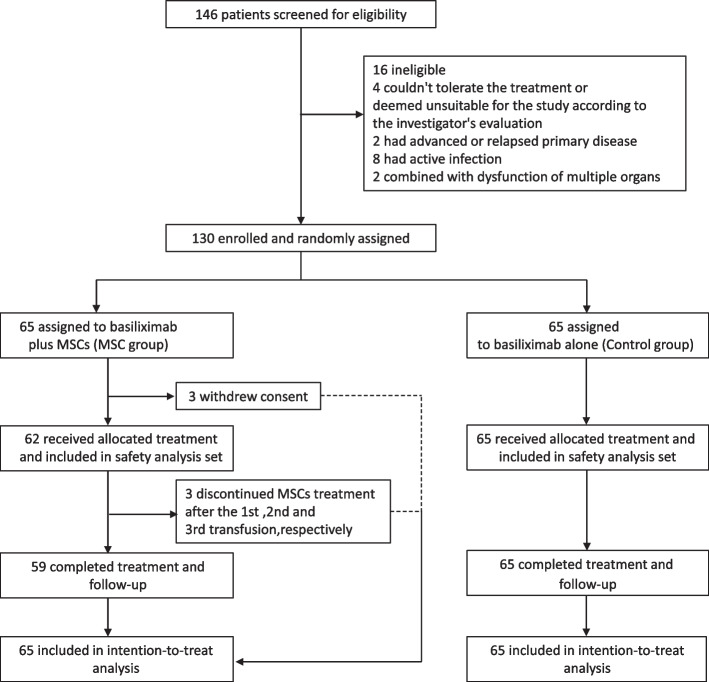
Methods: The primary endpoint of this multicentre, randomized, controlled trial was the 4-week complete response (CR) rate of SR-aGVHD. A total of 130 patients with SR-aGVHD were assigned in a 1:1 randomization schedule to the MSC group (receiving basiliximab plus MSCs) or control group (receiving basiliximab alone) (NCT04738981).
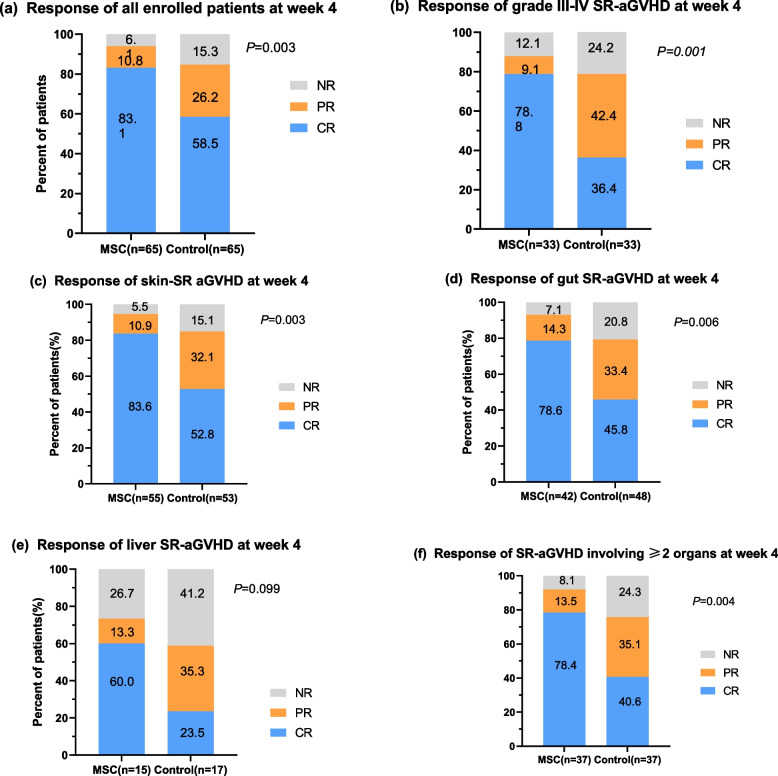
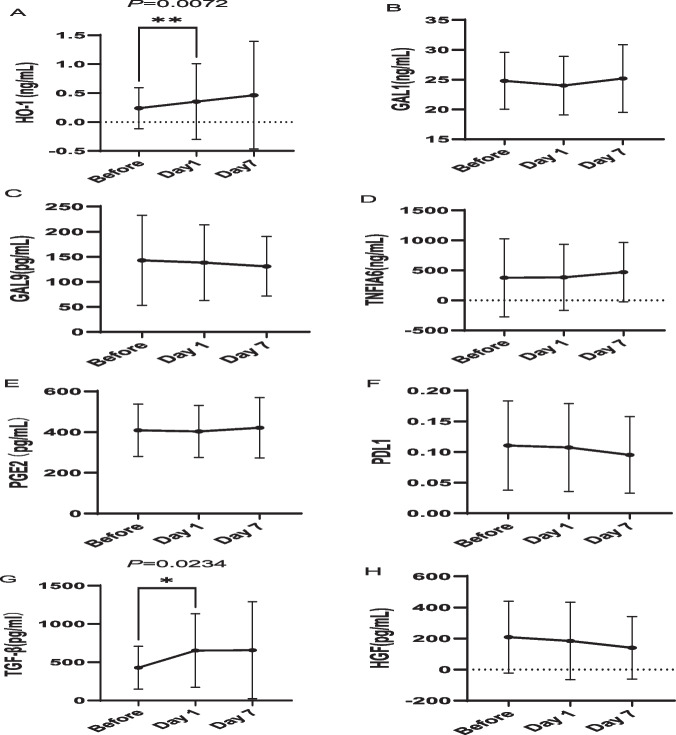
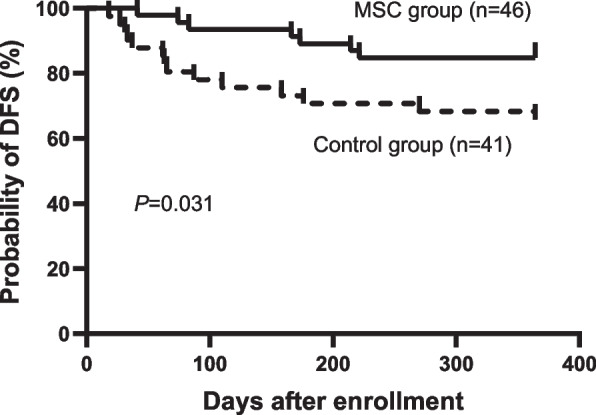
Results: Most enrolled patients (96.2%) received HID HSCT. The 4-week CR rate of SR-aGVHD in the MSC group was obviously better than that in the control group (83.1% vs. 55.4%, P = 0.001). However, for the overall response rates at week 4, the two groups were comparable. More patients in the control group used ≥ 6 doses of basiliximab (4.6% vs. 20%, P = 0.008). We collected blood samples from 19 consecutive patients and evaluated MSC-derived immunosuppressive cytokines, including HO1, GAL1, GAL9, TNFIA6, PGE2, PDL1, TGF-β and HGF. Compared to the levels before MSC infusion, the HO1 (P = 0.0072) and TGF-β (P = 0.0243) levels increased significantly 1 day after MSC infusion. At 7 days after MSC infusion, the levels of HO1, GAL1, TNFIA6 and TGF-β tended to increase; however, the differences were not statistically significant. Although the 52-week cumulative incidence of cGVHD in the MSC group was comparable to that in the control group, fewer patients in the MSC group developed cGVHD involving ≥3 organs (14.3% vs. 43.6%, P = 0.006). MSCs were well tolerated, no infusion-related adverse events (AEs) occurred and other AEs were also comparable between the two groups. However, patients with malignant haematological diseases in the MSC group had a higher 52-week disease-free survival rate than those in the control group (84.8% vs. 65.9%, P = 0.031).
Conclusions: For SR-aGVHD after allo-HSCT, especially HID HSCT, the combination of MSCs and basiliximab as the second-line therapy led to significantly better 4-week CR rates than basiliximab alone. The addition of MSCs not only did not increase toxicity but also provided a survival benefit.
Keywords: Acute graft-versus-host disease; Haemopoietic stem cell transplantation; Haploidentical; Mesenchymal stromal cells; Second-line therapy; Steroid-refractory.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Gratwohl A, Brand R, Frassoni F, Rocha V, Niederwieser D, Reusser P, Einsele H, Cordonnier C. Cause of death after allogeneic haematopoietic stem cell transplantation (HSCT) in early leukaemias: an EBMT analysis of lethal infectious complications and changes over calendar time. Bone Marrow Transplant. 2005;36(9):757–769. doi: 10.1038/sj.bmt.1705140. - DOI - PubMed
-
- Nagler A, Labopin M, Houhou M, Aljurf M, Mousavi A, Hamladji RM, Al ZM, Bondarenko S, Arat M, Angelucci E, et al. Outcome of haploidentical versus matched sibling donors in hematopoietic stem cell transplantation for adult patients with acute lymphoblastic leukemia: a study from the acute leukemia working party of the european society for blood and marrow transplantation. J Hematol Oncol. 2021;14(1):53. doi: 10.1186/s13045-021-01065-7. - DOI - PMC - PubMed
-
- Martin PJ, Rizzo JD, Wingard JR, Ballen K, Curtin PT, Cutler C, Litzow MR, Nieto Y, Savani BN, Schriber JR, et al. First- and second-line systemic treatment of acute graft-versus-host disease: recommendations of the American Society of Blood and Marrow Transplantation. Biol Blood Marrow Transplant. 2012;18(8):1150–1163. doi: 10.1016/j.bbmt.2012.04.005. - DOI - PMC - PubMed
-
- Penack O, Marchetti M, Ruutu T, Aljurf M, Bacigalupo A, Bonifazi F, Ciceri F, Cornelissen J, Malladi R, Duarte RF, et al. Prophylaxis and management of graft versus host disease after stem-cell transplantation for haematological malignancies: updated consensus recommendations of the European Society for Blood and Marrow Transplantation. Lancet Haematol. 2020;7(2):e157–e167. doi: 10.1016/S2352-3026(19)30256-X. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
