

A new in-hospital mortality prediction nomogram for intensive care unit patients with acute pancreatitis
- PMID: 38414456
- PMCID: PMC10895952
- DOI: 10.5114/aoms/170960
A new in-hospital mortality prediction nomogram for intensive care unit patients with acute pancreatitis
Abstract
Introduction: Acute pancreatitis (AP) is a prevalent inflammatory disease that can lead to severe abdominal pain and multiple organ failure, potentially resulting in pancreatic necrosis and persistent dysfunction. A nomogram prediction model was developed to accurately evaluate the prognosis and provide therapy guidance to AP patients.
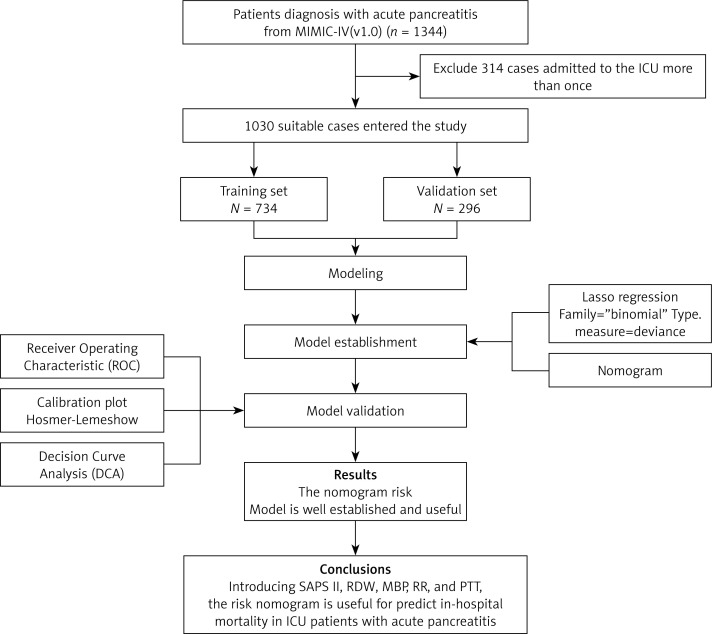
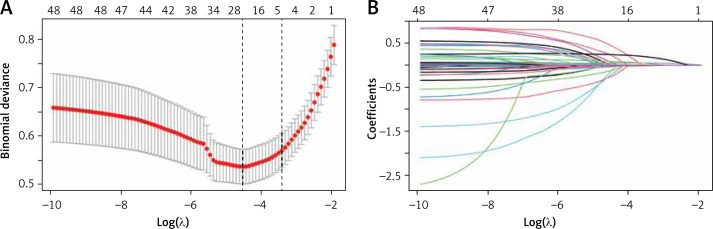
Material and methods: Retrospective data extraction was performed using MIMIC-IV, an open-source clinical database, to obtain 1344 AP patient records, of which the primary dataset included 1030 patients after the removal of repeated hospitalizations. The prediction of in-hospital mortality (IHM) used the least absolute shrinkage and selection operator (LASSO) regression model to optimize feature selection. A multivariate logistic regression analysis was used to build a prediction model incorporating the selected features, and the C-index, calibration plot, and decision curve analysis (DCA) were utilized to evaluate the discrimination, calibration, and clinical applicability of the prediction model.
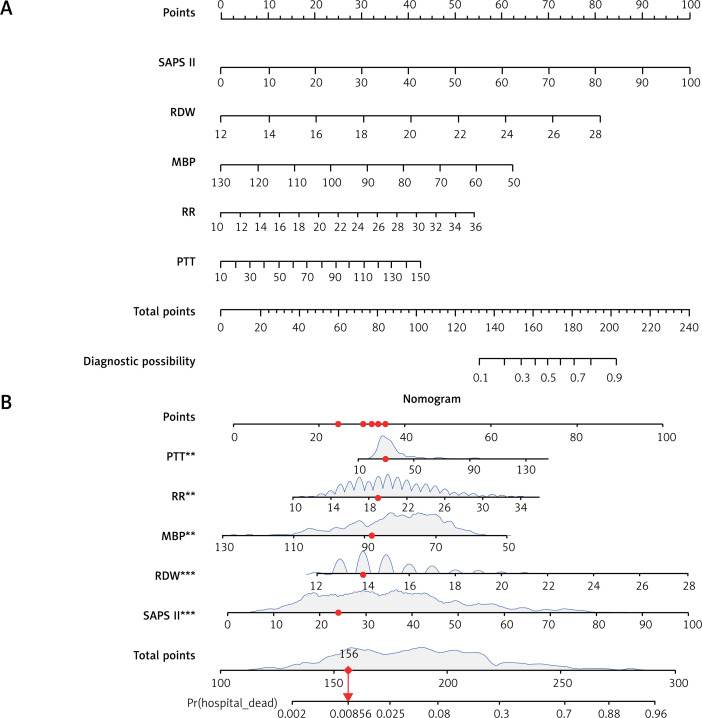
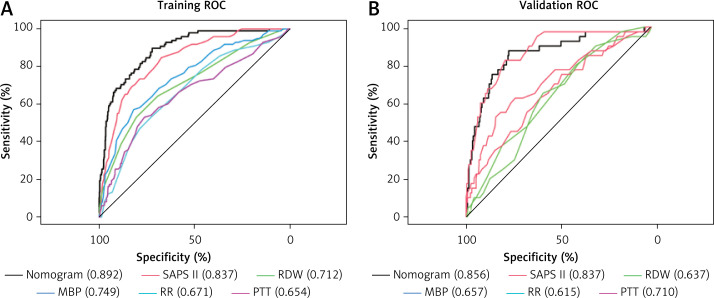
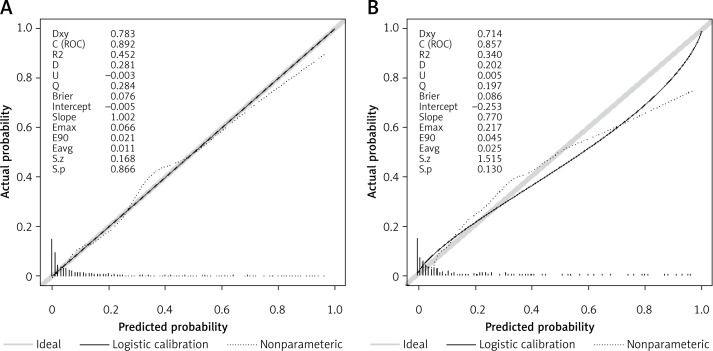
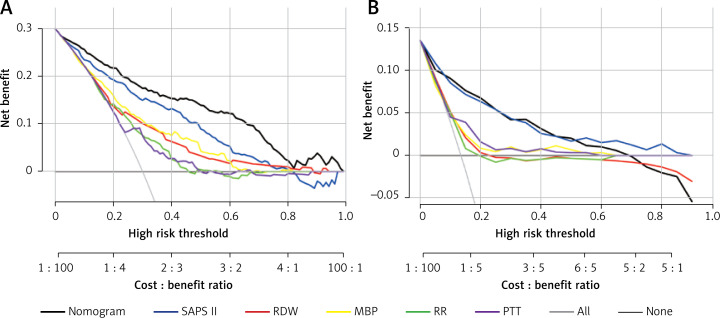
Results: The nomogram utilized a combination of indicators, including the SAPS II score, RDW, MBP, RR, PTT, and fluid-electrolyte disorders. Impressively, the model exhibited a satisfactory diagnostic performance, with area under the curve values of 0.892 and 0.856 for the training cohort and internal validation, respectively. Moreover, the calibration plots and the Hosmer-Lemeshow goodness-of-fit (HL) test revealed a strong correlation between the predicted and actual outcomes (p = 0.73), further confirming the reliability of our model. Notably, the results of the decision curve analysis (DCA) highlighted the superiority of our model over previously described scoring methods in terms of net clinical benefit, solidifying its value in clinical applications.
Conclusions: Our novel nomogram is a simple tool for accurately predicting IHM in ICU patients with AP. Treatment methods that enhance the factors involved in the model may contribute to increased in-hospital survival for these ICU patients.
Keywords: Medical Information Mart for Intensive Care IV (MIMIC-IV); acute pancreatitis; in-hospital mortality; nomogram; prediction model.
Copyright: © 2023 Termedia & Banach.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
[Establishment and evaluation of early in-hospital death prediction model for patients with acute pancreatitis in intensive care unit].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2023 Aug;35(8):865-869. doi: 10.3760/cma.j.cn121430-20220713-00660. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2023. PMID: 37593868 Chinese.
-
Development and Internal Validation of a Nomogram to Predict Mortality During the ICU Stay of Thoracic Fracture Patients Without Neurological Compromise: An Analysis of the MIMIC-III Clinical Database.Front Public Health. 2021 Dec 22;9:818439. doi: 10.3389/fpubh.2021.818439. eCollection 2021. Front Public Health. 2021. PMID: 35004604 Free PMC article.
-
Construction and validation of a risk assessment model for acute kidney injury in patients with acute pancreatitis in the intensive care unit.BMC Nephrol. 2023 Oct 26;24(1):315. doi: 10.1186/s12882-023-03369-x. BMC Nephrol. 2023. PMID: 37884898 Free PMC article.
-
Development and validation of a nomogram for predicting in-hospital mortality of patients with cervical spine fractures without spinal cord injury.Eur J Med Res. 2024 Jan 29;29(1):80. doi: 10.1186/s40001-024-01655-4. Eur J Med Res. 2024. PMID: 38287435 Free PMC article.
-
Development and Validation of a Dynamic Nomogram for Predicting in-Hospital Mortality in Patients with Acute Pancreatitis: A Retrospective Cohort Study in the Intensive Care Unit.Int J Gen Med. 2023 Jun 17;16:2541-2553. doi: 10.2147/IJGM.S409812. eCollection 2023. Int J Gen Med. 2023. PMID: 37351008 Free PMC article.
References
-
- Boxhoorn L, Voermans RP, Bouwense SA, et al. . Acute pancreatitis. Lancet 2020; 396: 726–34. - PubMed
-
- Iannuzzi JP, King JA, Leong JH, et al. . Global incidence of acute pancreatitis is increasing over time: a systematic review and meta-analysis. Gastroenterology 2022; 162: 122–34. - PubMed
-
- Roberts SE, Morrison-Rees S, John A, et al. . The incidence and aetiology of acute pancreatitis across Europe. Pancreatology 2017; 17: 155–65. - PubMed
-
- Banks PA, Bollen TL, Dervenis C, et al. . Acute Pancreatitis Classification Working Group . Classification of acute pancreatitis--2012: revision of the Atlanta classification and definitions by international consensus. Gut 2013; 62: 102–11. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous