

Endoscopic endonasal transsphenoidal surgery for unusual sellar lesions: eight cases and review of the literature
- PMID: 38414554
- PMCID: PMC10896968
- DOI: 10.3389/fneur.2024.1309691
Endoscopic endonasal transsphenoidal surgery for unusual sellar lesions: eight cases and review of the literature
Abstract
Background: Preoperative imaging for some unusual lesions in the sellar region can pose challenges in establishing a definitive diagnosis, impacting treatment strategies.
Methods: This study is a retrospective analysis of eight cases involving unusual sellar region lesions, all treated with endoscopic endonasal transsphenoidal surgery (EETS). We present the clinical, endocrine, and radiological characteristics, along with the outcomes of these cases.
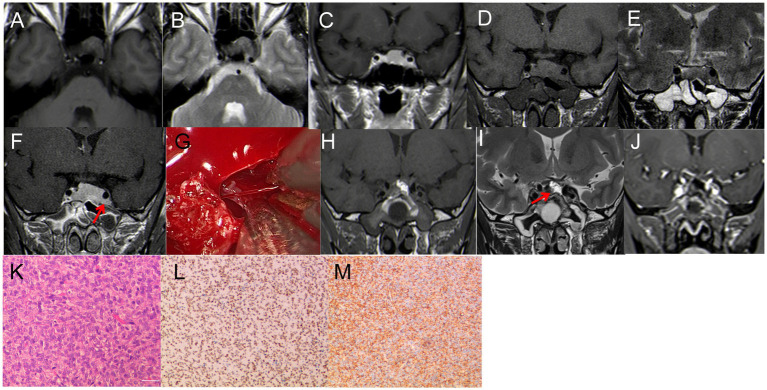
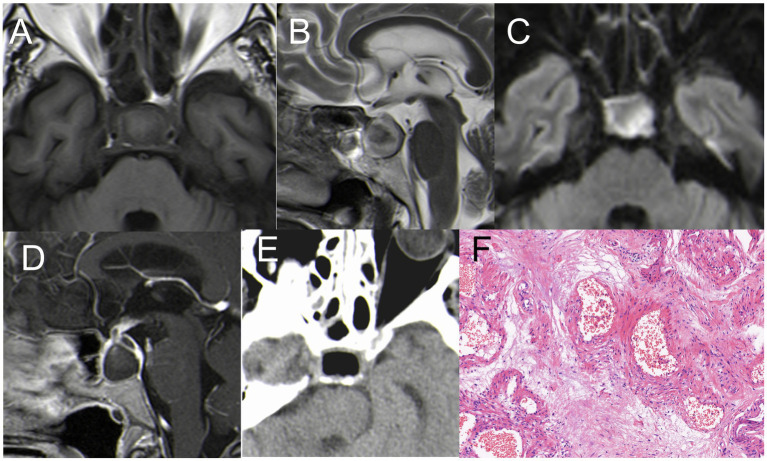
Results: Among the eight cases, the lesions were identified as follows: Solitary fibrous tumor (SFT) in one case, Lymphocytic hypophysitis (LYH) in one case, Cavernous sinus hemangiomas (CSH) in one case, Ossifying fibroma (OF) in two cases; Sphenoid sinus mucocele (SSM) in one case, Pituitary abscess (PA) in two cases. All patients underwent successful EETS, and their diagnoses were confirmed through pathological examination. Postoperatively, all patients had uneventful recoveries without occurrences of diabetes insipidus or visual impairment.
Conclusion: Our study retrospectively analyzed eight unusual lesions of the sellar region. Some lesions exhibit specific imaging characteristics and clinical details that can aid in preoperative diagnosis and inform treatment strategies for these unusual sellar diseases.
Keywords: Mucocele; cavernous sinus hemangiomas; endoscopic endonasal surgery; lymphocytic hypophysitis; ossifying fibroma; pituitary abscess; sellar lesions; solitary fibrous tumor.
Copyright © 2024 Wu, Deng, Qian, Lu, Ding, Hu, Gong, Tang and Ma.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures






References
LinkOut - more resources
Full Text Sources
Research Materials