

Orforglipron, a novel non-peptide oral daily glucagon-like peptide-1 receptor agonist as an anti-obesity medicine: A systematic review and meta-analysis
- PMID: 38414573
- PMCID: PMC10896246
- DOI: 10.1002/osp4.743
Orforglipron, a novel non-peptide oral daily glucagon-like peptide-1 receptor agonist as an anti-obesity medicine: A systematic review and meta-analysis
Abstract
Background: Orforglipron is a novel once-daily oral non-peptide glucagon-like peptide-1 receptor agonist with several recently published randomized controlled trials (RCTs) evaluating its role in diabetes and obesity. No meta-analysis has analyzed the efficacy and safety of orforglipron; this meta-analysis aimed to address this knowledge gap.
Methods: A systematic search was conducted in electronic databases to identify RCTs that included individuals with obesity who were administered orforglipron and compared to either a placebo or an active comparator. The primary outcome of interest was the percent change in body weight.
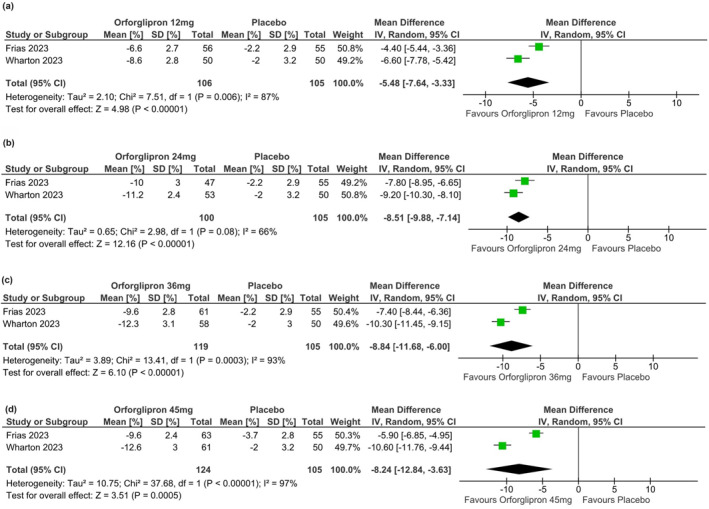
Results: From 12 initially screened articles, data from three RCTs involving 774 people were analyzed with a follow-up duration of up to 36 weeks. Compared to placebo, patients receiving orforglipron 12 mg/day (mean difference (MD), MD -5.48%, 95% CI [-7.64, -3.33], p < 0.01), 24 mg/day (MD -8.51%, 95% confidence interval (CI) [-9.88, -7.14], p < 0.01), 36 mg/day (MD -8.84%, 95% CI [-11.68, -6.00], p < 0.01) and 45 mg/day (MD -8.24%, 95% CI [-12.84, -3.63], p < 0.01) had a significantly greater percent reduction in body weight. The percentage of patients being able to achieve >15% weight loss from baseline was significantly higher with orforglipron 24 mg/day [Odds ratio (OR) 21.90 (95% CI [4.06, 118.15], p = 0.0003), 36 mg/day (OR 17.43, 95% CI [3.18, 95.66], p = 0.001) and 45 mg/day (OR 23.17, 95% CI [4.37, 123.03], p = 0.0002). Total but not severe adverse events were significantly higher with all the doses of orforglipron compared to placebo, with the hazard ratios being higher with higher doses. Gastrointestinal side-effects were predominant side effects, being dose-dependent, with nausea, vomiting, constipation, and gastroesophageal reflux being the predominant ones.
Conclusion: Orforglipron at 24-45 mg/day doses is an effective weight loss medication. The efficacy versus side effect profile suggests that 24-36 mg/day is the most optimal dose for orforglipron as an anti-obesity medicine.
Keywords: GLP1RA; emerging treatments; medications; obesity; orforglipron.
© 2024 The Authors. Obesity Science & Practice published by World Obesity and The Obesity Society and John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Garvey WT, Mechanick JI, Brett EM, et al. American Association of Clinical Endocrinologists and American College of Endocrinology comprehensive clinical practice guidelines for medical care of patients with obesity. Endocr Pract. 2016;22(suppl 3):1‐203. 10.4158/ep161365.gl - DOI - PubMed
-
- Dutta D, Jaisani R, Khandelwal D, Ghosh S, Malhotra R, Kalra S. Role of metformin, Sodium‐Glucose Cotransporter‐2 (SGLT2) Inhibitors, Glucagon‐Like Peptide‐1 (GLP‐1) receptor agonists, and orlistat based multidrug therapy in glycemic control, weight loss, and euglycemia in diabetes and obesity: a real‐world experience. Indian J Endocr Metab. 2019;23(4):460‐467. 10.4103/ijem.ijem_185_19 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous