

Small cell lung cancer with dermatomyositis: a case report
- PMID: 38414744
- PMCID: PMC10898245
- DOI: 10.3389/fonc.2024.1325991
Small cell lung cancer with dermatomyositis: a case report
Abstract
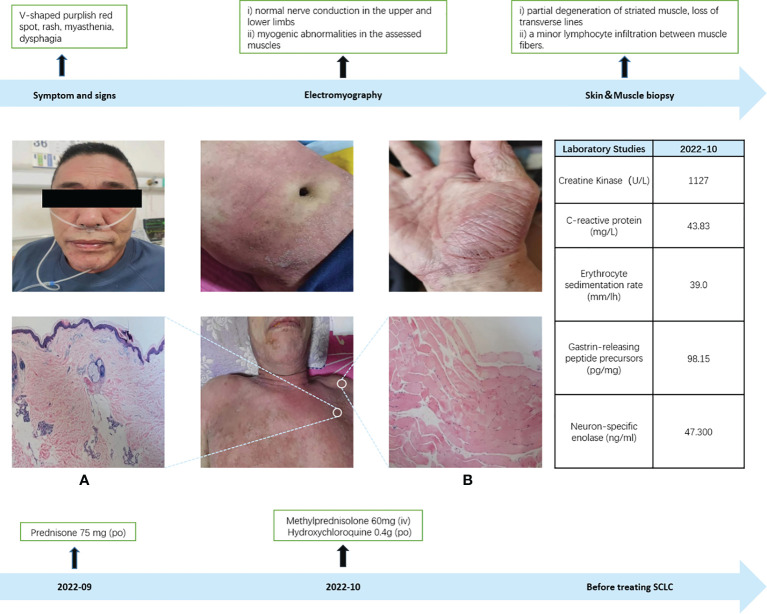
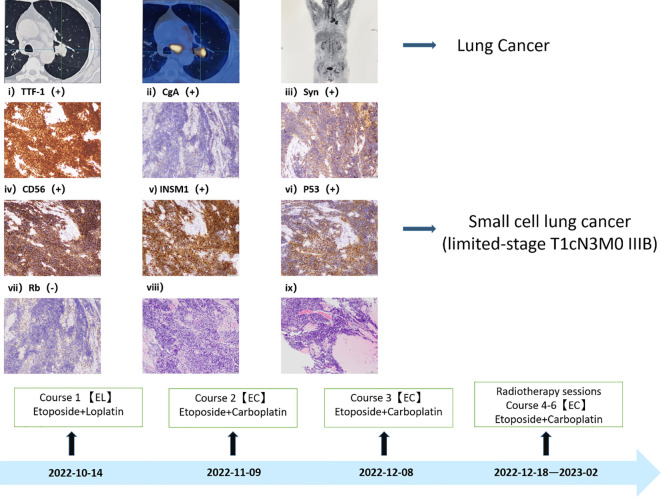
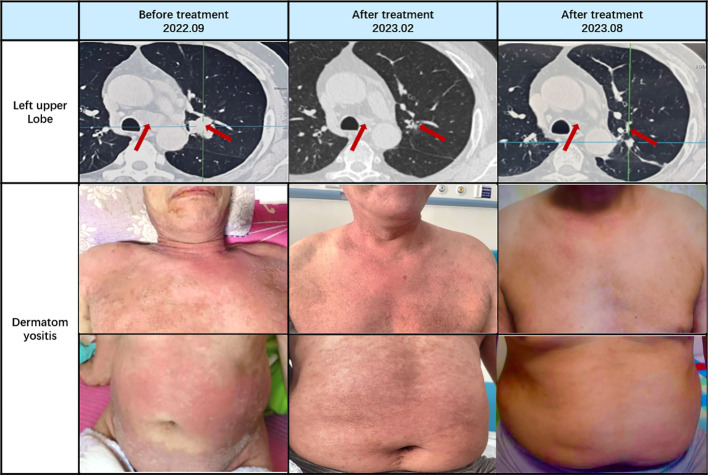
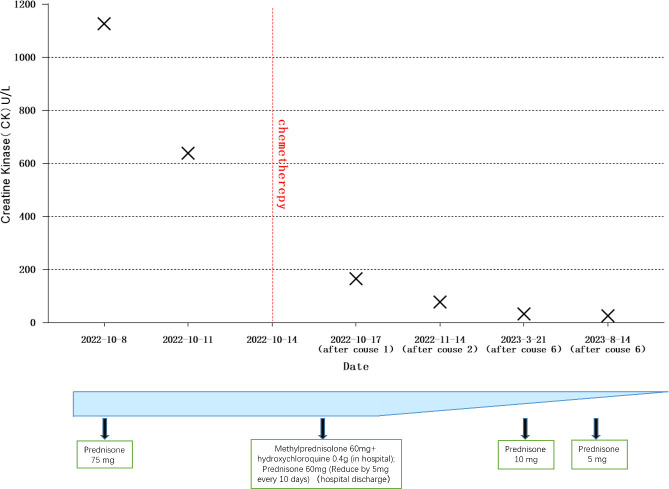
Dermatomyositis represents an autoimmune disorder characterized by notable skin and muscular manifestations. The annual incidence of dermatomyositis stands at approximately (5~10)/1 million individuals. Notably, patients with malignant tumors exhibit an elevated risk of developing dermatomyositis compared to the general population. However, in cases where dermatomyositis co-occurs with malignancy, the efficacy of hormone therapy alone tends to be suboptimal. Moreover, reports addressing the correlation between tumor treatment and the management of dermatomyositis are scarce. A 60-year-old male patient presented with dermatomyositis, initially manifesting through symptoms such as rash, muscle weakness, and dysphagia. Despite undergoing standard hormone therapy, there was no discernible improvement in the dermatomyositis symptoms. Considering the patient's concomitant troublesome cough, further investigations were conducted, including CT, PET-CT, and pathological biopsy. These assessments confirmed the diagnosis of limited-stage small cell lung cancer (T1cN3M0 IIIB). Notably, in this patient, dermatomyositis was suspected to be a paraneoplastic syndrome associated with small cell lung cancer. Standard chemotherapy and radiotherapy were employed to treat the small cell lung cancer, resulting in partial remission after two treatment cycles. As the malignancy regressed, a notable improvement in dermatomyositis symptoms was observed, subsequently leading to a gradual reduction in the prescribed hormone dosage. In conclusion, we present a comprehensive case study of dermatomyositis as a paraneoplastic syndrome throughout the treatment process. The response to tumor therapy coincided with the amelioration of dermatomyositis symptoms. Therefore, diligent malignancy screening is imperative for patients diagnosed with dermatomyositis.
Keywords: SCLC; dermatomyositis; lung cancer; paraneoplastic syndrome; small cell lung cancer.
Copyright © 2024 Guan, Qiu, Xu, Zu, Sun, Guo, Wang and Ma.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials