

Extensively drug-resistant Pseudomonas aeruginosa: clinical features and treatment with ceftazidime/avibactam and ceftolozane/tazobactam in a tertiary care university hospital center in Portugal - A cross-sectional and retrospective observational study
- PMID: 38414772
- PMCID: PMC10896734
- DOI: 10.3389/fmicb.2024.1347521
Extensively drug-resistant Pseudomonas aeruginosa: clinical features and treatment with ceftazidime/avibactam and ceftolozane/tazobactam in a tertiary care university hospital center in Portugal - A cross-sectional and retrospective observational study
Abstract
Introduction: Extensively drug-resistant Pseudomonas aeruginosa (XDR-PA) is a growing concern due to its increasing incidence, limited therapeutic options, limited data on the optimal treatment, and high mortality rates. The study aimed to characterize the population, the outcome and the microbiological characteristics of XDR-PA identified in a Portuguese university hospital center.
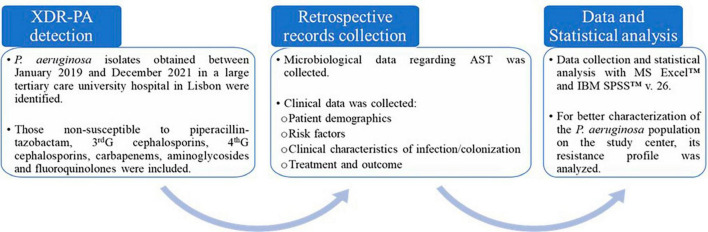
Methods: All XDR-PA isolates between January 2019 and December 2021 were identified. XDR-PA was defined as resistance to piperacillin-tazobactam, third and fourth generation cephalosporins, carbapenems, aminoglycosides and fluoroquinolones. A retrospective analysis of the medical records was performed.
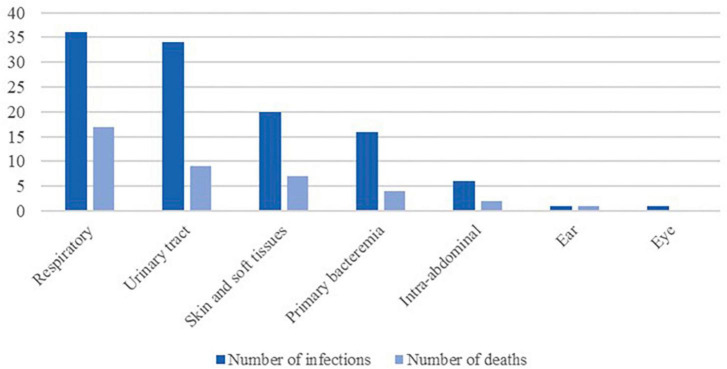
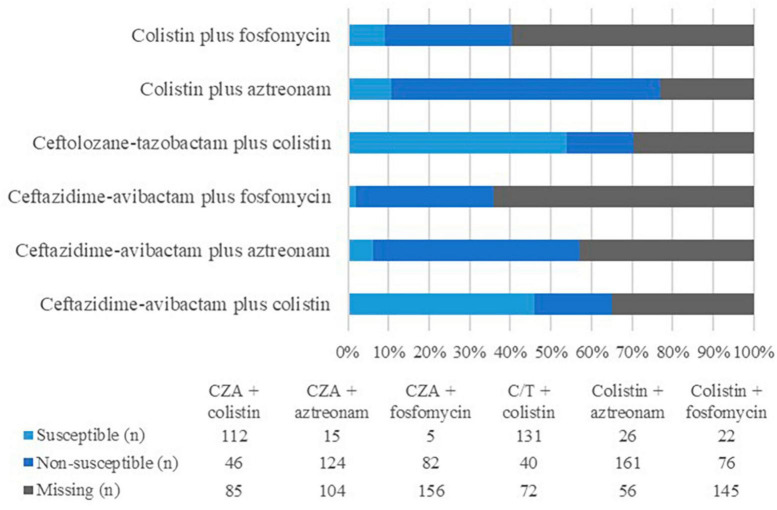
Results: One hundred seventy-eight individual episodes among 130 patients with XDR-PA detection were identified. The most common sources of infection were respiratory (32%) and urinary tracts (30%), although skin and soft tissue infections (18%) and primary bacteremia (14%) were also prevalent. Colonization was admitted in 64 cases. Several patients had risk factors for complicated infections, most notably immunosuppression, structural lung abnormalities, major surgery, hemodialysis or foreign intravascular or urinary devices. XDR-PA identification was more frequent in male patients with an average age of 64.3 ± 17.5 years. One non-susceptibility to colistin was reported. Only 12.4% were susceptible to aztreonam. Ceftazidime-avibactam (CZA) was susceptible in 71.5% of the tested isolates. Ceftolozane-tazobactam (C/T) was susceptible in 77.5% of the tested isolates. Antibiotic regimens with XDR-PA coverage were reserved for patients with declared infection, except to cystic fibrosis. The most frequently administered antibiotics were colistin (41 cases), CZA (39 cases), and C/T (16 cases). When combination therapy was used, CZA plus colistin was preferred. The global mortality rate among infected patients was 35.1%, significantly higher in those with hematologic malignancy (50.0%, p < 0.05), followed by the ones with bacteremia (44.4%, p < 0.05) and those medicated with colistin (39.0%, p < 0.05), especially the ones with respiratory infections (60.0%). Among patients treated with CZA or C/T, the mortality rate seemed to be lower.
Discussion: XDR-PA infections can be severe and difficult to treat, with a high mortality rate. Even though colistin seems to be a viable option, it is likely less safe and efficient than CZA and C/T. To the best of the authors' knowledge, this is the first description of the clinical infection characteristics and treatment of XDR-PA in Portugal.
Keywords: Pseudomonas aeruginosa; antimicrobial resistance; ceftazidime-avibactam; ceftolozane-tazobactam; difficult-to-treat infections; extensively drug-resistant.
Copyright © 2024 Mendes Pedro, Paulo, Santos, Fonseca, Melo Cristino, Pereira and Caneiras.
Conflict of interest statement
JM and CC received research grants administered through university and honoraria for serving on the speaker’s bureaus of Pfizer and MSD that were not related to the present study. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Ceftazidime/avibactam and ceftolozane/tazobactam for the treatment of extensively drug-resistant Pseudomonas aeruginosa post-neurosurgical infections: three cases and a review of the literature.Infection. 2021 Jun;49(3):549-553. doi: 10.1007/s15010-020-01539-9. Epub 2020 Oct 19. Infection. 2021. PMID: 33074365 Free PMC article. Review.
-
Combined Resistance to Ceftolozane-Tazobactam and Ceftazidime-Avibactam in Extensively Drug-Resistant (XDR) and Multidrug-Resistant (MDR) Pseudomonas aeruginosa: Resistance Predictors and Impact on Clinical Outcomes Besides Implications for Antimicrobial Stewardship Programs.Antibiotics (Basel). 2021 Oct 8;10(10):1224. doi: 10.3390/antibiotics10101224. Antibiotics (Basel). 2021. PMID: 34680805 Free PMC article.
-
Time-Kill Evaluation of Antibiotic Combinations Containing Ceftazidime-Avibactam against Extensively Drug-Resistant Pseudomonas aeruginosa and Their Potential Role against Ceftazidime-Avibactam-Resistant Isolates.Microbiol Spectr. 2021 Sep 3;9(1):e0058521. doi: 10.1128/Spectrum.00585-21. Epub 2021 Jul 28. Microbiol Spectr. 2021. PMID: 34319141 Free PMC article.
-
Aminoglycoside or Polymyxin Monotherapy for Treating Complicated Urinary Tract Infections Caused by Extensively Drug-Resistant Pseudomonas aeruginosa: A Propensity Score-Adjusted and Matched Cohort Study.Infect Dis Ther. 2022 Feb;11(1):335-350. doi: 10.1007/s40121-021-00570-z. Epub 2021 Dec 3. Infect Dis Ther. 2022. PMID: 34860333 Free PMC article.
-
Ceftolozane/tazobactam for difficult-to-treat Pseudomonas aeruginosa infections: A systematic review of its efficacy and safety for off-label indications.Int J Antimicrob Agents. 2020 Mar;55(3):105891. doi: 10.1016/j.ijantimicag.2020.105891. Epub 2020 Jan 8. Int J Antimicrob Agents. 2020. PMID: 31923569
Cited by
-
Case Report: Pan-Drug Resistant Pseudomonas aeruginosa from a Child with an Infected Burn Wound at the University Teaching Hospital of Kigali, Rwanda.Infect Drug Resist. 2024 Oct 25;17:4637-4642. doi: 10.2147/IDR.S486519. eCollection 2024. Infect Drug Resist. 2024. PMID: 39469095 Free PMC article.
-
Risk of Colonization with Multidrug-Resistant Gram-Negative Bacteria Among Travellers and Migrants: A Narrative Review.Trop Med Infect Dis. 2025 Jan 18;10(1):26. doi: 10.3390/tropicalmed10010026. Trop Med Infect Dis. 2025. PMID: 39852677 Free PMC article. Review.
-
The Role of blaOXA-101 and blaOXA-573 in Extensively Drug-Resistant/ Pan Drug-Resistant (XDR/PDR) Pseudomonas aeruginosa Resistance to Ceftazidime-Avibactam.Infect Drug Resist. 2025 May 16;18:2547-2555. doi: 10.2147/IDR.S506452. eCollection 2025. Infect Drug Resist. 2025. PMID: 40395970 Free PMC article.
-
Multidrug-resistant Pseudomonas aeruginosa in immunocompromised cancer patients: epidemiology, antimicrobial resistance, and virulence factors.BMC Infect Dis. 2025 Jun 11;25(1):804. doi: 10.1186/s12879-025-11182-0. BMC Infect Dis. 2025. PMID: 40500701 Free PMC article.
-
Activity of cefiderocol on extensively drug-resistant Pseudomonas aeruginosa from burn wound infections in Mansoura, Egypt.Iran J Microbiol. 2025 Apr;17(2):246-252. doi: 10.18502/ijm.v17i2.18384. Iran J Microbiol. 2025. PMID: 40337703 Free PMC article.
References
-
- Behzadi P., Ambrosi C., Scribano D., Zanetti S., Sarshar M., Gajdács M., et al. (2022a). Editorial: current perspectives on Pseudomonas aeruginosa: epidemiology, virulence and contemporary strategies to combat multidrug-resistant (MDR) pathogens. Front. Microbiol. 13:975616. 10.3389/fmicb.2022.975616 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources