

People living with HIV display increased anti-apolipoprotein A1 auto-antibodies, inflammation, and kynurenine metabolites: a case-control study
- PMID: 38414919
- PMCID: PMC10896987
- DOI: 10.3389/fcvm.2024.1343361
People living with HIV display increased anti-apolipoprotein A1 auto-antibodies, inflammation, and kynurenine metabolites: a case-control study
Abstract
Objective: This study aimed to study the relationship between auto-antibodies against apolipoprotein A1 (anti-apoA1 IgG), human immunodeficiency virus (HIV) infection, anti-retroviral therapy (ART), and the tryptophan pathways in HIV-related cardiovascular disease.
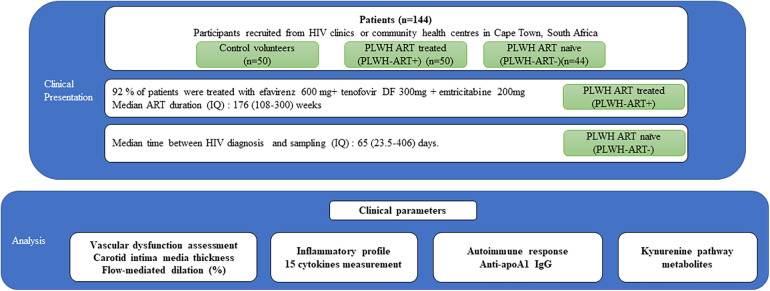
Design: This case-control study conducted in South Africa consisted of control volunteers (n = 50), people living with HIV (PLWH) on ART (n = 50), and untreated PLWH (n = 44). Cardiovascular risk scores were determined, vascular measures were performed, and an extensive biochemical characterisation (routine, metabolomic, and inflammatory systemic profiles) was performed.
Methods: Anti-apoA1 IgG levels were assessed by an in-house ELISA. Inflammatory biomarkers were measured with the Meso Scale Discovery® platform, and kynurenine pathway metabolites were assessed using targeted metabolomic profiling conducted by liquid chromatography-multiple reaction monitoring/mass spectrometry (LC-MRM/MS).
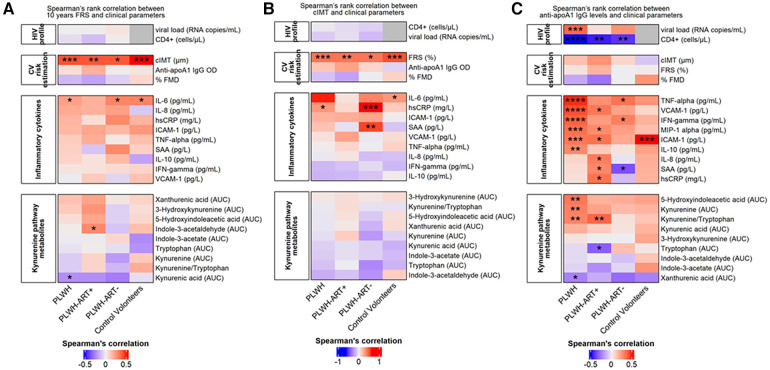
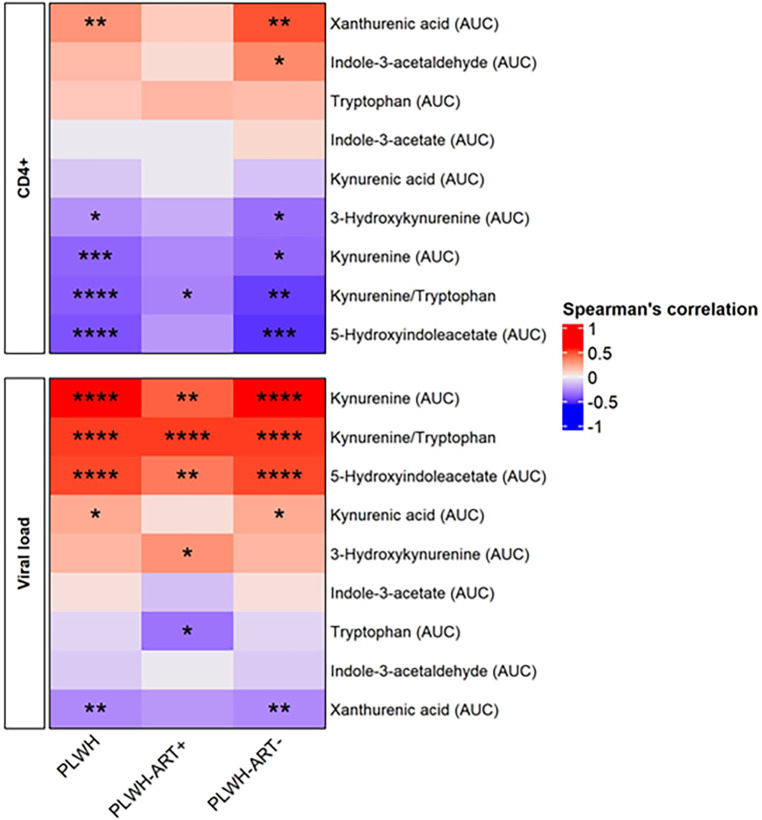
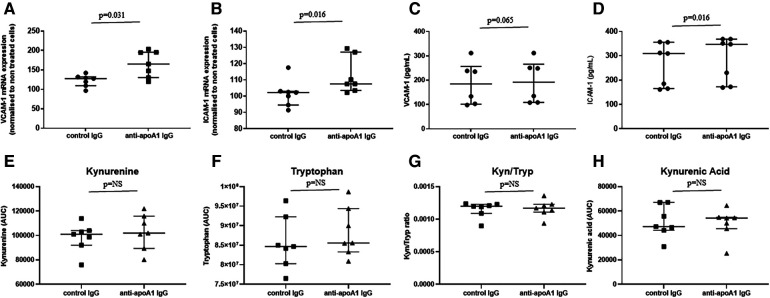
Results: Cardiovascular risk scores and vascular measures exhibited similarities across the three groups, while important differences were observed in systemic inflammatory and tryptophan pathways. Anti-apoA1 IgG seropositivity rates were 15%, 40%, and 70% in control volunteers, PLWH ART-treated, and PLWH ART-naïve, respectively. Circulating anti-apoA1 IgG levels were significantly negatively associated with CD4+ cell counts and positively associated with viremia and pro-inflammatory biomarkers (IFNγ, TNFα, MIPα, ICAM-1, VCAM-1). While circulating anti-apoA1 IgG levels were associated with increased levels of kynurenine in both control volunteers and PLWH, the kynurenine/tryptophan ratio was significantly increased in PLWH ART-treated.
Conclusion: HIV infection increases the humoral response against apoA1, which is associated with established HIV severity criteria and kynurenine pathway activation.
Keywords: HIV; anti-apolipoprotein A1 auto-antibodies; anti-retroviral therapy; autoimmunity; cardiovascular disease; kynurenine pathway metabolites.
© 2024 Frias, Pagano, Bararpour, Sidibé, Kamau, Fétaud-Lapierre, Hudson, Thomas, Lecour, Strijdom and Vuilleumier.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Lorgis L, Cottenet J, Molins G, Benzenine E, Zeller M, Aube H, et al. Outcomes after acute myocardial infarction in HIV-infected patients: analysis of data from a French nationwide hospital medical information database. Circulation. (2013) 127(17):1767–74. 10.1161/CIRCULATIONAHA.113.001874 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous