

Application of conventional ultrasound coupled with shear wave elastography in the assessment of muscle strength in patients with type 2 diabetes
- PMID: 38415110
- PMCID: PMC10895149
- DOI: 10.21037/qims-23-1152
Application of conventional ultrasound coupled with shear wave elastography in the assessment of muscle strength in patients with type 2 diabetes
Abstract
Background: In patients with type 2 diabetes mellitus (T2DM), a decrease in muscle function may be related to changes in the biomechanical properties of skeletal muscles. However, the correlations between muscle function and the characteristics of muscle size and stiffness as measured by ultrasound in patients with T2DM are unclear. The aim of this study was to investigate the abilities of conventional ultrasound and shear wave elastography (SWE) to assess muscle properties in patients with T2DM and to correlate the findings with isokinetic muscle testing and functional tests.
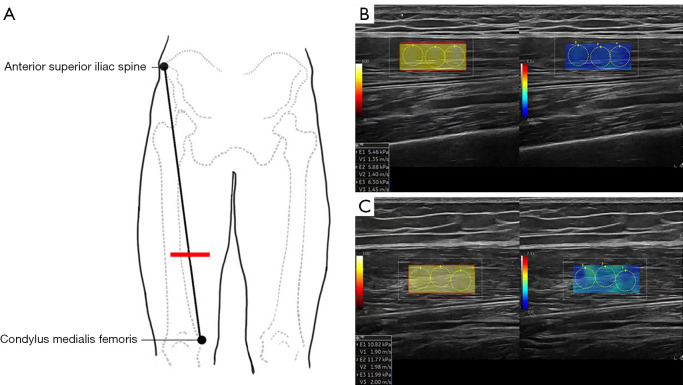
Methods: Sixty patients from the Department of Endocrinology in The Third Affiliated Hospital of Southern Medical University diagnosed with T2DM were recruited in this cross-sectional study from September 2021 to September 2022. T2DM was defined based on the American Diabetes Association criteria. The exclusion criteria were a history of injury or operation of the lower limb or clinical signs of neuromuscular disorders, any muscle-induced disease, and the presence of other types of diabetes mellitus. Thirty-five matched healthy volunteers were continuously included in the control group. SWE was used to measure the muscle stiffness of the quadriceps femoris [vastus lateralis (VL), rectus femoris (RF), vastus medialis (VM), vastus intermedius (VI)] and the biceps brachii (BB) in a relaxed position, and the shear wave velocity (SWV) values were recorded. Muscle size was measured using conventional ultrasound. The participants underwent isokinetic knee extension/flexion (60°/sec) to assess muscle strength and functional tests of physical performance, including the short physical performance battery, 30-s chair stand test, timed up-and-go test, and 6-meter walk test. All demographics and measured variables were compared using the independent samples t-test. Interclass correlation coefficient analysis was performed on the measurement data obtained by the two operators, and Pearson correlation coefficients were used to determine the relationships between variables.
Results: Patients with T2DM exhibited worse physical performance (P<0.05) and weaker lower limb muscle strength (P<0.05) than did healthy controls, but their handgrip strength was comparable (P=0.102). Patients with T2DM had significantly decreased muscle thickness [RF thickness: 10.69±3.21 vs. 13.09±2.41 mm, mean difference =-2.40, 95% confidence interval (CI): -3.56 to -1.24, P<0.001; anterior quadriceps thickness: 23.45±7.11 vs. 27.25±5.25 mm, mean difference =-3.80, 95% CI: -6.33 to -1.26, P=0.004] and RF cross-sectional area (3.04±1.10 vs. 4.11±0.95 cm2, mean difference =-1.07, 95% CI: -1.49 to -0.64; P<0.001) compared to healthy controls. Smaller muscle size was associated with decreased muscle strength (r=0.44-0.69, all P values <0.001). Except for the BB (3.48±0.38 vs. 3.61±0.61 m/s, mean difference =-0.12, 95% CI: -0.35 to 0.11; P=0.257) and VI (2.59±0.34 vs. 2.52±0.23 m/s, mean difference =0.03, 95% CI: -0.06 to 0.18; P=0.299), the muscle stiffness in patients with T2DM was significantly decreased. For the patients with T2DM and healthy participants, the SWV of the RF was 1.66±0.23 and 1.83±0.18 m/s (mean difference =-0.17, 95% CI: -0.25 to -0.08; P<0.001), respectively; that of the VM was 1.34±0.15 and 1.51±0.16 m/s (mean difference =-0.17, 95% CI: -0.24 to -0.10; P<0.001), respectively; and that of VL was 1.38±0.19 and 1.53±0.19 m/s (mean difference =-0.15, 95% CI: -0.23 to -0.07; P<0.001), respectively. Excellent interobserver reliability of the SWV measurements on the muscle of T2DM patients was observed (all intraclass correlation coefficients >0.75; P<0.001). The SWV showed moderate correlations with muscle strength in the RF, VM, and VL (r=0.30-0.61; all P values <0.05).
Conclusions: Ultrasound technology exhibits good reliability for repeated measurements of muscle size and stiffness. Reduced muscle stiffness as detected by SWE was demonstrated in patients with diabetes and was associated with decreased muscle strength and impaired functional activity.
Keywords: Muscle strength; isokinetic muscle testing; shear wave elastography (SWE); type 2 diabetes mellitus (T2DM); ultrasound.
2024 Quantitative Imaging in Medicine and Surgery. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://qims.amegroups.com/article/view/10.21037/qims-23-1152/coif). The authors have no conflicts of interest to declare.
Figures


Similar articles
-
Muscle shear wave elastography in idiopathic inflammatory myopathies: a case-control study with MRI correlation.Skeletal Radiol. 2019 Aug;48(8):1209-1219. doi: 10.1007/s00256-019-03175-3. Epub 2019 Feb 27. Skeletal Radiol. 2019. PMID: 30810778 Free PMC article.
-
Quantitative assessment of muscle properties in polymyositis and dermatomyositis using high-frequency ultrasound and shear wave elastography.Quant Imaging Med Surg. 2023 Jan 1;13(1):428-440. doi: 10.21037/qims-22-423. Epub 2022 Nov 22. Quant Imaging Med Surg. 2023. PMID: 36620135 Free PMC article.
-
Application of ultrasound elastography in the evaluation of muscle strength in a healthy population.Quant Imaging Med Surg. 2020 Oct;10(10):1961-1972. doi: 10.21037/qims-20-439. Quant Imaging Med Surg. 2020. PMID: 33014728 Free PMC article.
-
Reliability of Ultrasound Assessment of Hamstring Morphology, Quality, and Stiffness Among Healthy Adults and Athletes: A Systematic Review.J Sport Rehabil. 2024 Jul 19;33(6):396-415. doi: 10.1123/jsr.2023-0204. Print 2024 Aug 1. J Sport Rehabil. 2024. PMID: 39032922
-
Utility of ultrasound in measuring quadriceps muscle thickness in patients receiving maintenance hemodialysis: comprehensive systematic review and meta-analysis.Clin Exp Nephrol. 2025 Feb;29(2):192-211. doi: 10.1007/s10157-024-02557-9. Epub 2024 Oct 4. Clin Exp Nephrol. 2025. PMID: 39365526
References
-
- Bassi-Dibai D, Santos-de-Araújo AD, Dibai-Filho AV, de Azevedo LFS, Goulart CDL, Luz GCP, Burke PR, Garcia-Araújo AS, Borghi-Silva A. Rehabilitation of Individuals With Diabetes Mellitus: Focus on Diabetic Myopathy. Front Endocrinol (Lausanne) 2022;13:869921. 10.3389/fendo.2022.869921 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources