

Effect of moderate-intensity statin on carotid intraplaque neovascularization of coronary artery disease: a retrospective cohort study
- PMID: 38415148
- PMCID: PMC10895147
- DOI: 10.21037/qims-23-1104
Effect of moderate-intensity statin on carotid intraplaque neovascularization of coronary artery disease: a retrospective cohort study
Abstract
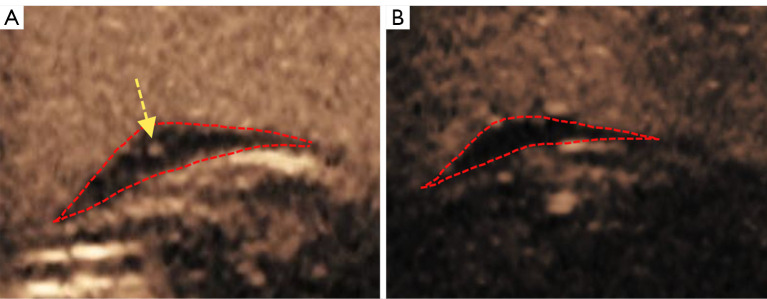
Background: Statin treatment can reduce atherosclerotic plaque as detected via invasive intracoronary methods. However, few studies have evaluated the effect of moderate-intensity statin therapy on carotid intraplaque neovascularization (IPN) using semiquantitative indices. This study thus aimed to assess the effect of statin on the carotid IPN of coronary artery disease with contrast-enhanced ultrasound (CEUS).
Methods: In this noncontrol, retrospective, cohort study, 35 inpatients who underwent coronary angiography, serial CEUS, and laboratory evaluations were consecutively enrolled from June 2020 to December 2022 at the Department of Cardiology, Chinese PLA General Hospital. All patients were administered moderate-intensity statin during serial CEUS, and continuous and categorical assessment of IPN and maximum plaque height (MPH) of carotid plaque was performed. Patients with a target low-density lipoprotein cholesterol (LDL-C) <1.8 mmol/L at 12-month follow-up were compared with those who did not reach the LDL-C 1.8 mmol/L target.
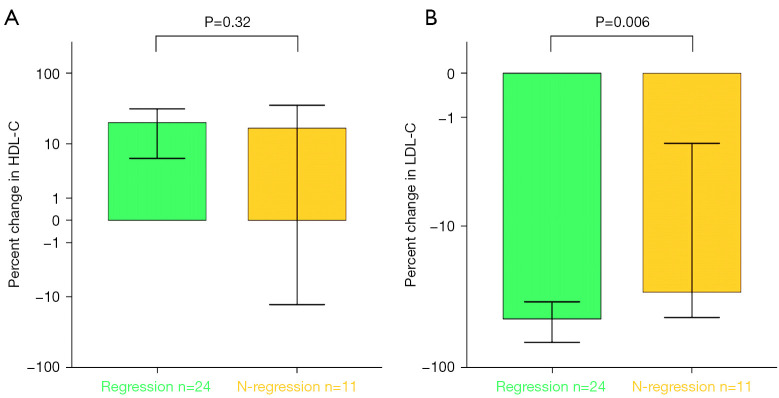
Results: From baseline to 12-month follow-up, there were significant differences in the LDL-C levels between patients (2.71±1.29 vs. 1.35±0.83 mmol/L), those with 12-month follow-up LDL-C <1.8 mmol/L (2.58±1.24 vs. 1.08±0.52 mmol/L), and those with 12-month follow-up LDL-C ≥1.8 mmol/L (3.24±1.44 vs. 2.56±0.85 mmol/L) all P values <0.05, with decreases of 41%, 49%, and 11% from baseline, respectively. The mean MPH (12 months to baseline) decreased from 2.47±0.63 to 2.22±0.60 mm (P<0.05), and the IPN also decreased from 1.15±0.62 to 0.58±0.56, representing a reduction of 0.57±0.59 from baseline (P<0.001). In the LDL-C <1.8 mmol/L patients, there were significant differences between baseline and 12 months in MPH (2.37±0.56 vs. 2.03±0.52 mm; P<0.05) and IPN (1.32±0.77 vs. 0.54±0.63; P<0.05) compared with those with a follow-up LDL-C ≥1.8 mmol/L. Patients with a follow-up LDL-C <1.8 mmol/L, compared with those with a follow-up LDL-C ≥1.8 mmol/L, showed a significantly greater reduction in MPH (-0.34±0.46 vs. -0.13±0.39; P<0.05) and IPN (-0.79±0.63 vs. -0.57±0.79; P<0.05). Additionally, patients with carotid IPN regression showed a higher percent change in LDL-C compared with those without carotid IPN regression (-53.31±23.20 vs. -29.55±19.47; P<0.05).
Conclusions: Controlling the LDL-C to <1.8 mmol/L under moderate-intensity statin can stabilize and reduce carotid IPN as detected by the semiquantitative noninvasive CEUS.
Keywords: Contrast-enhanced ultrasound (CEUS); coronary artery disease (CAD); intraplaque neovascularization (IPN); low-density lipoprotein cholesterol (LDL-C); moderate-intensity statin.
2024 Quantitative Imaging in Medicine and Surgery. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://qims.amegroups.com/article/view/10.21037/qims-23-1104/coif). The authors have no conflicts of interest to declare.
Figures


Similar articles
-
Effect of combining evolocumab with statin on carotid intraplaque neovascularization in patients with premature coronary artery disease (EPOCH).Atherosclerosis. 2024 Apr;391:117471. doi: 10.1016/j.atherosclerosis.2024.117471. Epub 2024 Feb 13. Atherosclerosis. 2024. PMID: 38493669
-
Effect of evolocumab on the progression of intraplaque neovascularization of the carotid based on contrast-enhanced ultrasonography (EPIC study): A prospective single-arm, open-label study.Front Pharmacol. 2023 Jan 4;13:999224. doi: 10.3389/fphar.2022.999224. eCollection 2022. Front Pharmacol. 2023. PMID: 36686711 Free PMC article.
-
Relationship Between Serum Lipid Profiles and Carotid Intraplaque Neovascularization in a High-Stroke-Risk Population: A Cross-Sectional Study in China.J Am Heart Assoc. 2021 Nov 16;10(22):e021545. doi: 10.1161/JAHA.121.021545. Epub 2021 Nov 10. J Am Heart Assoc. 2021. PMID: 34755547 Free PMC article.
-
Remnant Cholesterol and Carotid Intraplaque Neovascularization Assessed by Contrast-Enhanced Ultrasonography in Patients With Ischemic Stroke.Cardiol Res. 2024 Jun;15(3):144-152. doi: 10.14740/cr1634. Epub 2024 Jun 25. Cardiol Res. 2024. PMID: 38994226 Free PMC article.
-
Contrast-Enhanced Ultrasound to Assess Carotid Intraplaque Neovascularization.Ultrasound Med Biol. 2020 Mar;46(3):466-478. doi: 10.1016/j.ultrasmedbio.2019.10.020. Epub 2019 Nov 29. Ultrasound Med Biol. 2020. PMID: 31791553
References
-
- Baigent C, Blackwell L, Emberson J, Holland LE, Reith C, Bhala N, Peto R, Barnes EH, Keech A, Simes J, Collins R. Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet 2010;376:1670-81. 10.1016/S0140-6736(10)61350-5 - DOI - PMC - PubMed
-
- Pedersen TR, Faergeman O, Kastelein JJ, Olsson AG, Tikkanen MJ, Holme I, Larsen ML, Bendiksen FS, Lindahl C, Szarek M, Tsai J, Incremental Decrease in End Points Through Aggressive Lipid Lowering (IDEAL) Study Group . High-dose atorvastatin vs usual-dose simvastatin for secondary prevention after myocardial infarction: the IDEAL study: a randomized controlled trial. JAMA 2005;294:2437-45. 10.1001/jama.294.19.2437 - DOI - PubMed
-
- Grundy SM, Stone NJ, Bailey AL, Beam C, Birtcher KK, Blumenthal RS, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019;139:e1082-143. 10.1161/CIR.0000000000000625 - DOI - PMC - PubMed
-
- de Lemos JA, Blazing MA, Wiviott SD, Lewis EF, Fox KA, White HD, Rouleau JL, Pedersen TR, Gardner LH, Mukherjee R, Ramsey KE, Palmisano J, Bilheimer DW, Pfeffer MA, Califf RM, Braunwald E; Investigators. Early intensive vs a delayed conservative simvastatin strategy in patients with acute coronary syndromes: phase Z of the A to Z trial. JAMA 2004;292:1307-16. 10.1001/jama.292.11.1307 - DOI - PubMed
-
- Giugliano RP, Cannon CP, Blazing MA, Nicolau JC, Corbalán R, Špinar J, Park JG, White JA, Bohula EA, Braunwald E; IMPROVE-IT (Improved Reduction of Outcomes: Vytorin Efficacy International Trial) Investigators. Benefit of Adding Ezetimibe to Statin Therapy on Cardiovascular Outcomes and Safety in Patients With Versus Without Diabetes Mellitus: Results From IMPROVE-IT (Improved Reduction of Outcomes: Vytorin Efficacy International Trial). Circulation 2018;137:1571-82. 10.1161/CIRCULATIONAHA.117.030950 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous