

Cognition and Memory after Covid-19 in a Large Community Sample
- PMID: 38416429
- PMCID: PMC7615803
- DOI: 10.1056/NEJMoa2311330
Cognition and Memory after Covid-19 in a Large Community Sample
Abstract
Background: Cognitive symptoms after coronavirus disease 2019 (Covid-19), the disease caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), are well-recognized. Whether objectively measurable cognitive deficits exist and how long they persist are unclear.
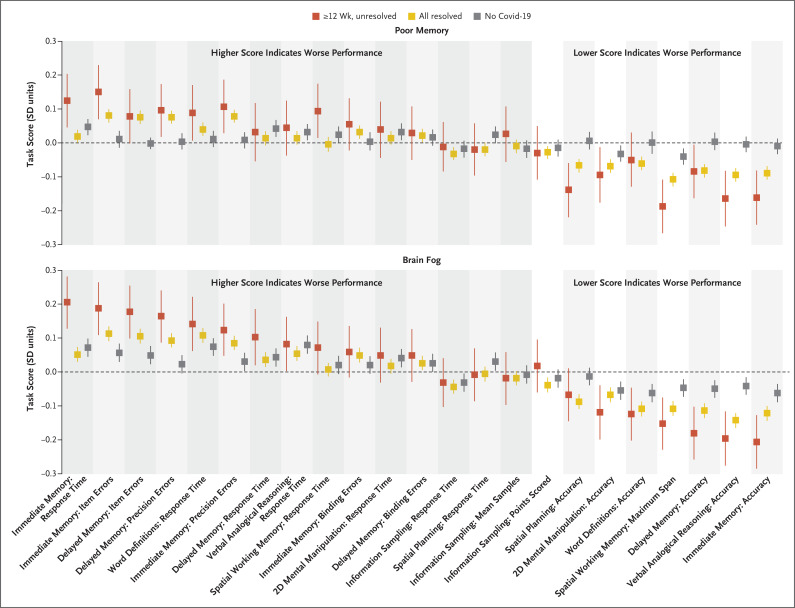
Methods: We invited 800,000 adults in a study in England to complete an online assessment of cognitive function. We estimated a global cognitive score across eight tasks. We hypothesized that participants with persistent symptoms (lasting ≥12 weeks) after infection onset would have objectively measurable global cognitive deficits and that impairments in executive functioning and memory would be observed in such participants, especially in those who reported recent poor memory or difficulty thinking or concentrating ("brain fog").
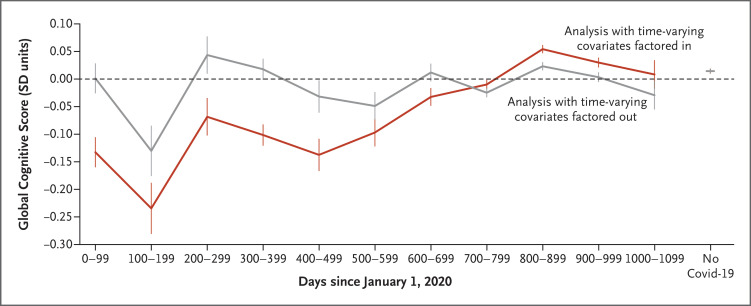
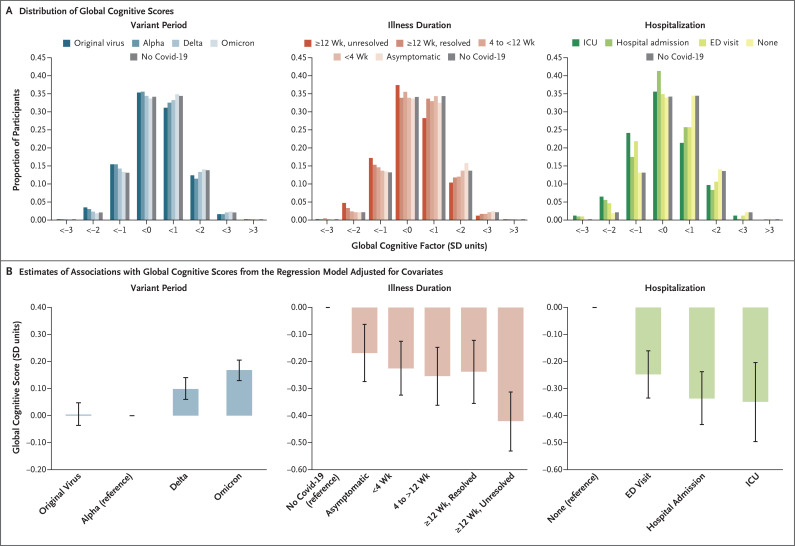
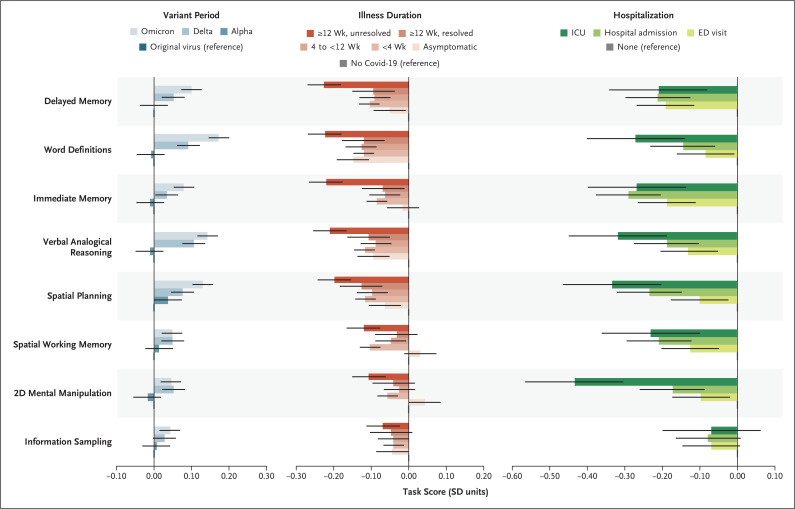
Results: Of the 141,583 participants who started the online cognitive assessment, 112,964 completed it. In a multiple regression analysis, participants who had recovered from Covid-19 in whom symptoms had resolved in less than 4 weeks or at least 12 weeks had similar small deficits in global cognition as compared with those in the no-Covid-19 group, who had not been infected with SARS-CoV-2 or had unconfirmed infection (-0.23 SD [95% confidence interval {CI}, -0.33 to -0.13] and -0.24 SD [95% CI, -0.36 to -0.12], respectively); larger deficits as compared with the no-Covid-19 group were seen in participants with unresolved persistent symptoms (-0.42 SD; 95% CI, -0.53 to -0.31). Larger deficits were seen in participants who had SARS-CoV-2 infection during periods in which the original virus or the B.1.1.7 variant was predominant than in those infected with later variants (e.g., -0.17 SD for the B.1.1.7 variant vs. the B.1.1.529 variant; 95% CI, -0.20 to -0.13) and in participants who had been hospitalized than in those who had not been hospitalized (e.g., intensive care unit admission, -0.35 SD; 95% CI, -0.49 to -0.20). Results of the analyses were similar to those of propensity-score-matching analyses. In a comparison of the group that had unresolved persistent symptoms with the no-Covid-19 group, memory, reasoning, and executive function tasks were associated with the largest deficits (-0.33 to -0.20 SD); these tasks correlated weakly with recent symptoms, including poor memory and brain fog. No adverse events were reported.
Conclusions: Participants with resolved persistent symptoms after Covid-19 had objectively measured cognitive function similar to that in participants with shorter-duration symptoms, although short-duration Covid-19 was still associated with small cognitive deficits after recovery. Longer-term persistence of cognitive deficits and any clinical implications remain uncertain. (Funded by the National Institute for Health and Care Research and others.).
Copyright © 2024 Massachusetts Medical Society.
Figures
Comment in
-
Cognition and Memory after Covid-19 in a Large Community Sample.N Engl J Med. 2024 Jun 6;390(21):2034. doi: 10.1056/NEJMc2403996. N Engl J Med. 2024. PMID: 38838322 Free PMC article. No abstract available.
-
Cognition and Memory after Covid-19 in a Large Community Sample.N Engl J Med. 2024 Jun 6;390(21):2034-2035. doi: 10.1056/NEJMc2403996. N Engl J Med. 2024. PMID: 38838323 No abstract available.
-
Cognition and Memory after Covid-19 in a Large Community Sample. Reply.N Engl J Med. 2024 Jun 6;390(21):2035. doi: 10.1056/NEJMc2403996. N Engl J Med. 2024. PMID: 38838324 No abstract available.
-
Kognitive Defizite auch nach leichter Covid-Erkrankung.MMW Fortschr Med. 2024 Aug;166(13):22-23. doi: 10.1007/s15006-024-4134-6. MMW Fortschr Med. 2024. PMID: 39112859 German. No abstract available.
References
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous