

Outcomes of Women Undergoing Noncardiac Surgery in Veterans Affairs Compared With Non-Veterans Affairs Care Settings
- PMID: 38416481
- PMCID: PMC10902781
- DOI: 10.1001/jamasurg.2023.8081
Outcomes of Women Undergoing Noncardiac Surgery in Veterans Affairs Compared With Non-Veterans Affairs Care Settings
Abstract
Importance: Recent legislation facilitates veterans' ability to receive non-Veterans Affairs (VA) surgical care. Although veterans are predominantly male, the number of women receiving care within the VA has nearly doubled to 10% over the past decade and recent data comparing the surgical care of women in VA and non-VA care settings are lacking.
Objective: To compare postoperative outcomes among women treated in VA hospitals vs private-sector hospitals.
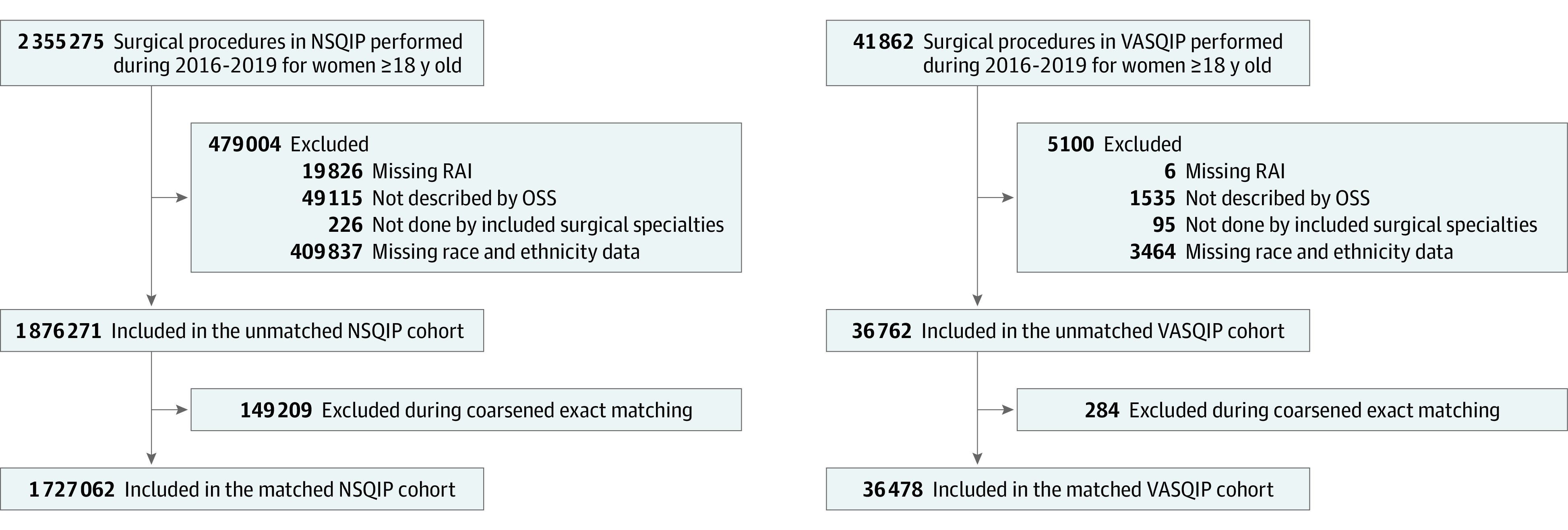
Design, setting, and participants: This coarsened exact-matched cohort study across 9 noncardiac specialties in the Veterans Affairs Surgical Quality Improvement Program (VASQIP) and American College of Surgeons National Surgical Quality Improvement Program (NSQIP) took place from January 1, 2016, to December 31, 2019. Multivariable Poisson models with robust standard errors were used to evaluate the association between VA vs private-sector care settings and 30-day mortality. Hospitals participating in American College of Surgeons NSQIP and VASQIP were included. Data analysis was performed in January 2023. Participants included female patients 18 years old or older.
Exposures: Surgical care in VA or private-sector hospitals.
Main outcomes and measures: Postoperative 30-day mortality and failure to rescue (FTR).
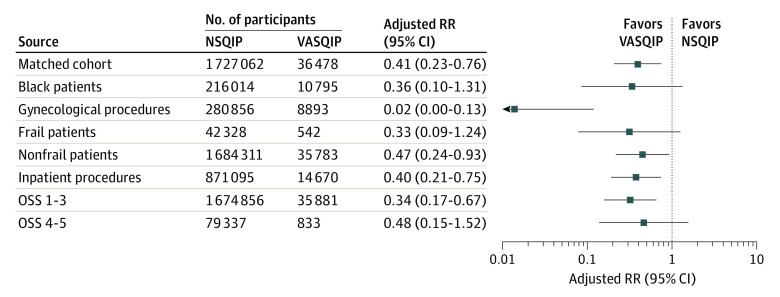
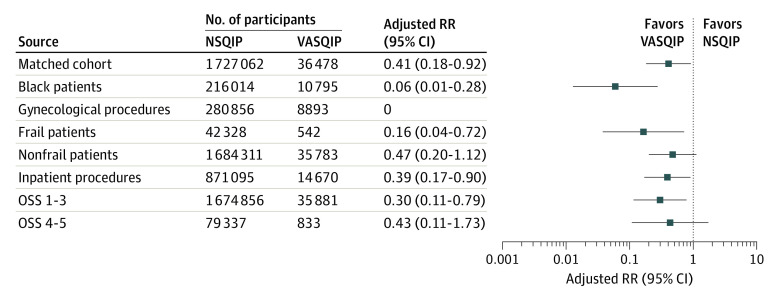
Results: Among 1 913 033 procedures analyzed, patients in VASQIP were younger (VASQIP: mean age, 49.8 [SD, 13.0] years; NSQIP: mean age, 55.9 [SD, 16.9] years; P < .001) and although most patients in both groups identified as White, there were significantly more Black women in VASQIP compared with NSQIP (29.6% vs 12.7%; P < .001). The mean risk analysis index score was lower in VASQIP (13.9 [SD, 6.4]) compared with NSQIP (16.3 [SD, 7.8]) (P < .001 for both). Patients in the VA were more likely to have a preoperative acute serious condition (2.4% vs 1.8%: P < .001), but cases in NSQIP were more frequently emergent (6.9% vs 2.6%; P < .001). The 30-day mortality, complications, and FTR were 0.2%, 3.2%, and 0.1% in VASQIP (n = 36 762 procedures) as compared with 0.8%, 5.0%, and 0.5% in NSQIP (n = 1 876 271 procedures), respectively (all P < .001). Among 1 763 540 matched women (n = 36 478 procedures in VASQIP; n = 1 727 062 procedures in NSQIP), these rates were 0.3%, 3.7%, and 0.2% in NSQIP and 0.1%, 3.4%, and 0.1% in VASQIP (all P < .01). Relative to private-sector care, VA surgical care was associated with a lower risk of death (adjusted risk ratio [aRR], 0.41; 95% CI, 0.23-0.76). This finding was robust among women undergoing gynecologic surgery, inpatient surgery, and low-physiologic stress procedures. VA surgical care was also associated with lower risk of FTR (aRR, 0.41; 95% CI, 0.18-0.92) for frail or Black women and inpatient and low-physiologic stress procedures.
Conclusions and relevance: Although women comprise the minority of veterans receiving care within the VA, in this study, VA surgical care for women was associated with half the risk of postoperative death and FTR. The VA appears better equipped to meet the unique surgical needs and risk profiles of veterans, regardless of sex and health policy decisions, including funding, should reflect these important outcome differences.
Conflict of interest statement
Figures
Comment on
-
The MISSION Act Needs Measurement.JAMA Surg. 2024 May 1;159(5):509-510. doi: 10.1001/jamasurg.2023.8082. JAMA Surg. 2024. PMID: 38416508 No abstract available.
References
-
- US Department of Veterans Affairs . Veterans Health Administration. Accessed January 25, 2024. https://www.va.gov/health/aboutvha.asp
-
- National Archives . Veterans Community Care Program. Accessed January 25, 2024. https://www.federalregister.gov/documents/2019/06/05/2019-11575/veterans...
-
- US Congress . Veterans Access, Choice, and Accountability Act of 2014. Accessed January 25, 2024. https://www.congress.gov/bill/113th-congress/house-bill/3230
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
