

Relationship between maternal obesity and first-trimester TSH in women with negative anti-TPO antibodies
- PMID: 38417259
- PMCID: PMC11046355
- DOI: 10.1530/ETJ-23-0213
Relationship between maternal obesity and first-trimester TSH in women with negative anti-TPO antibodies
Abstract
Objective: Obesity is associated with increased thyroid-stimulating hormone (TSH) in non-pregnant subjects, but this phenomenon has not been fully characterized during pregnancy. Our aim was to evaluate the impact of BMI on first-trimester TSH in a wide cohort of pregnant women with negative anti-thyroperoxidase antibodies (AbTPO) and its implications on uterine artery pulsatility index (UtA-PI), a marker of early placentation.
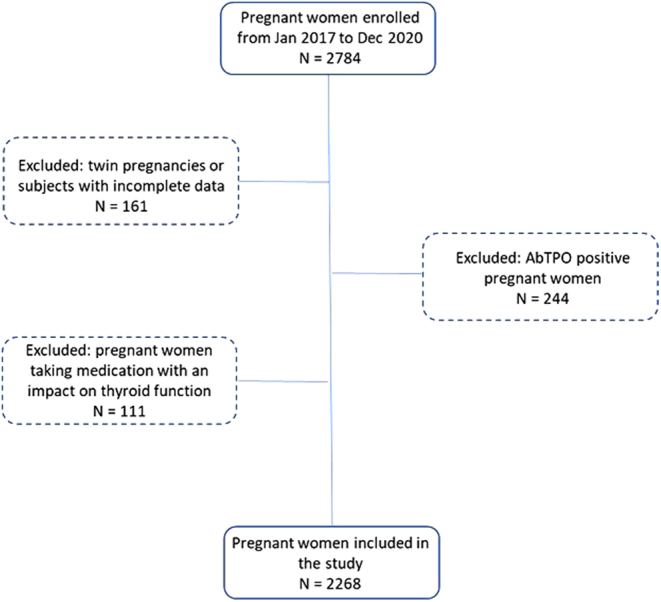
Methods: The study included 2268 AbTPO-negative pregnant women at their first antenatal visit. Anamnestic data, BMI, TSH, anti-nuclear antibody (ANA) and extractable nuclear antigen (ENA) positivity and mean UtA-PI were collected.
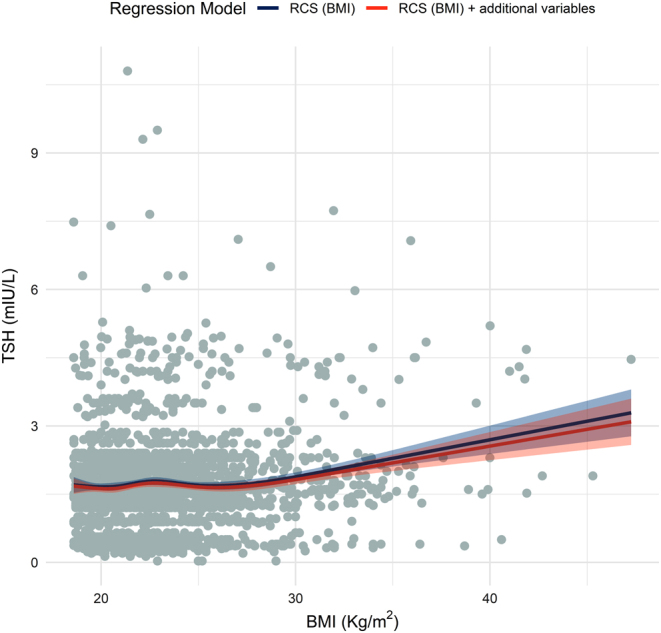
Results: A total of 1693 women had normal weight, 435 were overweight and 140 were obese. Maternal age, ANA/ENA positivity, history of autoimmune diseases and familiar history of thyroid diseases were similar in the three groups. TSH was significantly higher in obese women (1.8 (IQR: 1.4-2.4) mU/L) when compared to normal weight (1.6 (IQR: 1.2-2.2) mU/L) and overweight (median: 1.6 (IQR: 1.2-2.2) mU/L) ones (P < 0.001). BMI was significantly related with the risk of having a TSH level ≥4 mU/L at logistic regression, independently from non-thyroid autoimmunity, smoking or familiar predisposition for thyroid diseases (OR: 1.125, 95% CI: 1.080-1.172, P < 0.001). A restricted cubic splines regression showed a non-linear relationship between BMI and TSH. Women with a TSH ≥4 mU/L had a higher UtA-PI, independently from BMI.
Conclusion: Overweight/obesity is significantly related with TSH serum levels in AbTPO-negative pregnant women, independently from the other risk factors for hypothyroidism during pregnancy. The increase of TSH levels could be clinically relevant, as suggested by its association with abnormal UtA-PI, a surrogate marker of abnormal placentation.
Keywords: TSH; hypothyroidism; obesity; pregnancy; thyroid.
Conflict of interest statement
The authors declare that there is no conflict of interest that could be perceived as prejudicing the impartiality of the study reported.
Figures
Similar articles
-
A first-trimester serum TSH in the 4-10 mIU/L range is associated with obstetric complications in thyroid peroxidase antibody-negative women.J Endocrinol Invest. 2023 Jul;46(7):1407-1414. doi: 10.1007/s40618-022-01996-z. Epub 2022 Dec 23. J Endocrinol Invest. 2023. PMID: 36562959
-
Optimization of the follow-up of pregnant women with autoimmune thyroid disease.Endocrinol Diabetes Nutr (Engl Ed). 2019 May;66(5):305-311. doi: 10.1016/j.endinu.2018.08.011. Epub 2018 Nov 16. Endocrinol Diabetes Nutr (Engl Ed). 2019. PMID: 30455046 English, Spanish.
-
[Comparison of the effect of different diagnostic criteria of subclinical hypothyroidism and positive TPO-Ab on pregnancy outcomes].Zhonghua Fu Chan Ke Za Zhi. 2014 Nov;49(11):824-8. Zhonghua Fu Chan Ke Za Zhi. 2014. PMID: 25603906 Chinese.
-
Association of Thyroid Function Test Abnormalities and Thyroid Autoimmunity With Preterm Birth: A Systematic Review and Meta-analysis.JAMA. 2019 Aug 20;322(7):632-641. doi: 10.1001/jama.2019.10931. JAMA. 2019. PMID: 31429897 Free PMC article.
-
Association between maternal thyroid function and risk of gestational hypertension and pre-eclampsia: a systematic review and individual-participant data meta-analysis.Lancet Diabetes Endocrinol. 2022 Apr;10(4):243-252. doi: 10.1016/S2213-8587(22)00007-9. Epub 2022 Mar 4. Lancet Diabetes Endocrinol. 2022. PMID: 35255260 Free PMC article.
References
-
- Alexander EK, Pearce EN, Brent GA, Brown RS, Chen H, Dosiou C, Grobman WA, Laurberg P, Lazarus JH, Mandel SJ, et al.2017 Guidelines of the American Thyroid Association for the diagnosis and management of thyroid disease during pregnancy and the postpartum. Thyroid 201727315–389. (10.1089/thy.2016.0457) - DOI - PubMed
-
- Rotondi M Chiovato L Pacini F Bartalena L & Vitti P. Management of subclinical hypothyroidism in pregnancy: a comment from the Italian society of endocrinology and the Italian Thyroid Association to the 2017 American Thyroid Association guidelines-"the Italian way". Thyroid 201828551–555. (10.1089/thy.2017.0424) - DOI - PubMed
-
- Magri F Bellingeri C De Maggio I Croce L Coperchini F Rotondi M Chiovato L Spinillo A & Beneventi F. A first-trimester serum TSH in the 4–10 mIU/L range is associated with obstetric complications in thyroid peroxidase antibody-negative women. Journal of Endocrinological Investigation 2023461407–1414. (10.1007/s40618-022-01996-z) - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
