

A case of peripheral T-cell lymphoma in which therapy-related myelodysplastic syndrome developed and a second autologous transplantation was performed
- PMID: 38417872
- PMCID: PMC11079989
- DOI: 10.3960/jslrt.23054
A case of peripheral T-cell lymphoma in which therapy-related myelodysplastic syndrome developed and a second autologous transplantation was performed
Abstract
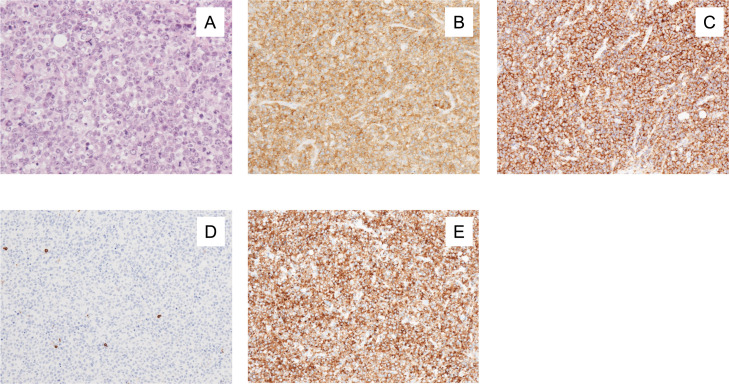
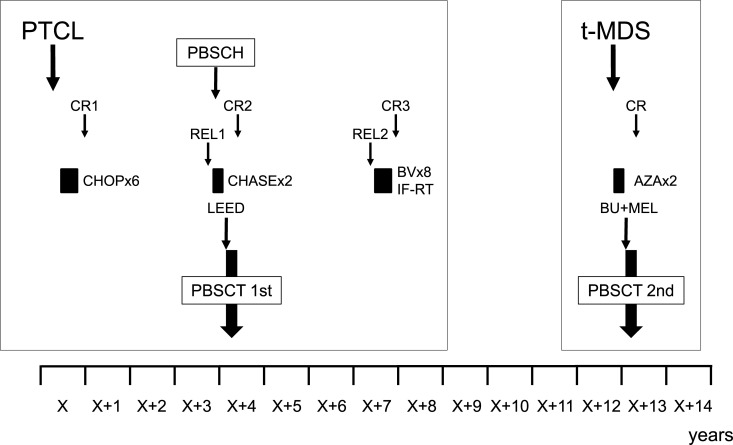
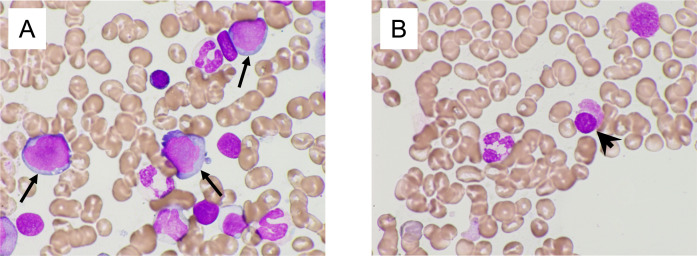
We report a case of therapy-related myelodysplastic syndrome (MDS), which developed 9 years after autologous peripheral blood stem cell transplantation (PBSCT) for peripheral T-cell lymphoma, not otherwise specified (PTCL-NOS). A 65-year-old male was diagnosed with PTCL-NOS. After 6 cycles of the CHOP (cyclophosphamide [CPA], doxorubicin, vincristine, and prednisone) regimen, he achieved a first complete response (CR). He relapsed 33 months later and received salvage chemotherapy, which consisted of the CHASE regimen (CPA, high-dose cytarabine, dexamethasone, and etoposide). During the recovery phase of the first cycle of CHASE, his peripheral blood stem cells (PBSCs) were harvested and frozen in 2 bags. After 2 courses of CHASE, he underwent autologous PBSCT, which involved the use of the LEED preconditioning regimen (melphalan, CPA, etoposide, and dexamethasone) and one of the frozen bags. This resulted in a second CR. At 39 months after PBSCT, he relapsed with a tumor in his right arm. After it was resected, he received eight cycles of brentuximab vedotin and 45 Gy of involved-field irradiation concurrently and achieved a third CR. Nine years after autologous PBSCT, he was diagnosed with MDS with excess blasts 2 (MDS-EB-2). His disease progressed to acute myeloid leukemia after 2 courses of azacitidine therapy. He successfully underwent a second autologous PBSCT involving the busulfan and melphalan preconditioning regimen and the other frozen bag, which had been stored for 9 years. He has been in complete cytogenetic remission for 1 year since the second autologous PBSCT.
Keywords: autologous peripheral blood stem cell transplantation; peripheral T-cell lymphoma, not otherwise specified; therapy-related myelodysplastic syndrome.
Conflict of interest statement
CONFLICT OF INTEREST
The authors declare that they have no conflicts of interest.
Figures
Similar articles
-
Peripheral T-cell lymphoma: the role of hematopoietic stem cell transplantation.Crit Rev Oncol Hematol. 2014 Feb;89(2):248-61. doi: 10.1016/j.critrevonc.2013.08.016. Epub 2013 Sep 8. Crit Rev Oncol Hematol. 2014. PMID: 24075060 Review.
-
Intensive chemotherapy (high-dose CHOP/ESHAP regimen) followed by autologous stem-cell transplantation in previously untreated patients with peripheral T-cell lymphoma.Ann Oncol. 2008 May;19(5):958-63. doi: 10.1093/annonc/mdn022. Epub 2008 Feb 25. Ann Oncol. 2008. PMID: 18303032 Clinical Trial.
-
A case of treatment-related myelodysplastic syndrome and acute myelogenous leukemia following high-dose chemotherapy with autologous stem cell transplantation for non-Hodgkin's lymphoma.J Korean Med Sci. 2002 Aug;17(4):555-9. doi: 10.3346/jkms.2002.17.4.555. J Korean Med Sci. 2002. PMID: 12172056 Free PMC article.
-
DexaBEAM versus ICE salvage regimen prior to autologous transplantation for relapsed or refractory aggressive peripheral T cell lymphoma: a retrospective evaluation of parallel patient cohorts of one center.Ann Hematol. 2013 Aug;92(8):1041-8. doi: 10.1007/s00277-013-1738-9. Epub 2013 Mar 27. Ann Hematol. 2013. PMID: 23532626
-
Treatment of relapsed aggressive lymphomas: regimens with and without high-dose therapy and stem cell rescue.Cancer Chemother Pharmacol. 2002 May;49 Suppl 1:S13-20. doi: 10.1007/s00280-002-0447-1. Epub 2002 Apr 12. Cancer Chemother Pharmacol. 2002. PMID: 12042984 Review.
References
-
- Vose J, Armitage J, Weisenburger D. International T-Cell Lymphoma Project. International peripheral T-cell and natural killer/T-cell lymphoma study: pathology findings and clinical outcomes. J Clin Oncol. 2008; 26: 4124-4130. - PubMed
-
- Cazzola M. Myelodysplastic Syndromes. N Engl J Med. 2020; 383: 1358-1374. - PubMed
-
- Swerdlow SH. International Agency for Research on C: WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. 4th ed, Lyon, International Agency for Research on Cancer. 2017.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous