

Validation of body surface colonic mapping (BSCM) against high resolution colonic manometry for evaluation of colonic motility
- PMID: 38418514
- PMCID: PMC10902299
- DOI: 10.1038/s41598-024-54429-7
Validation of body surface colonic mapping (BSCM) against high resolution colonic manometry for evaluation of colonic motility
Abstract
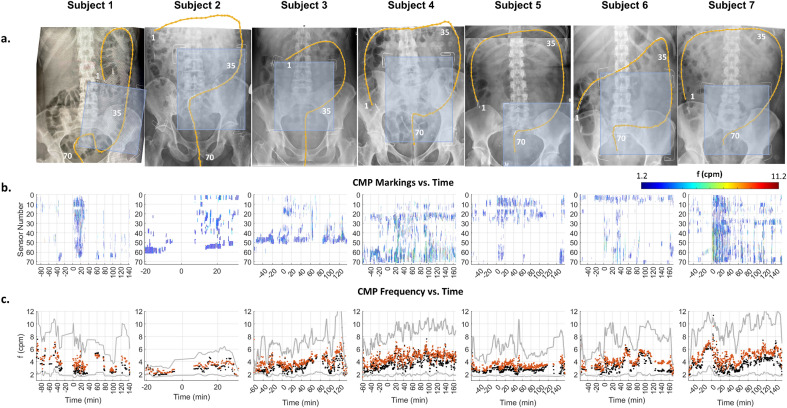
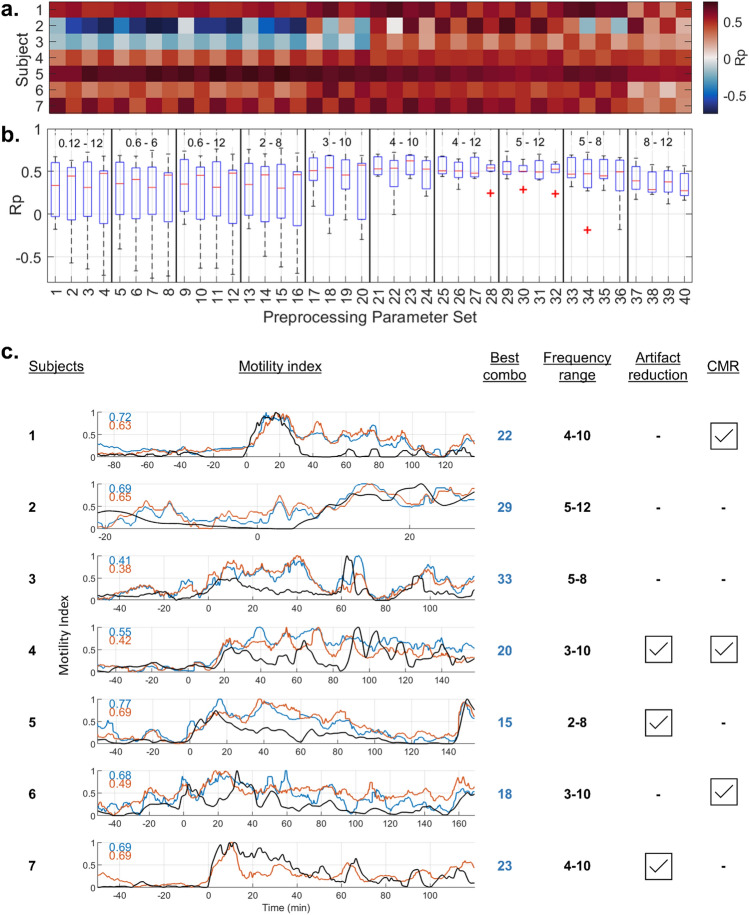
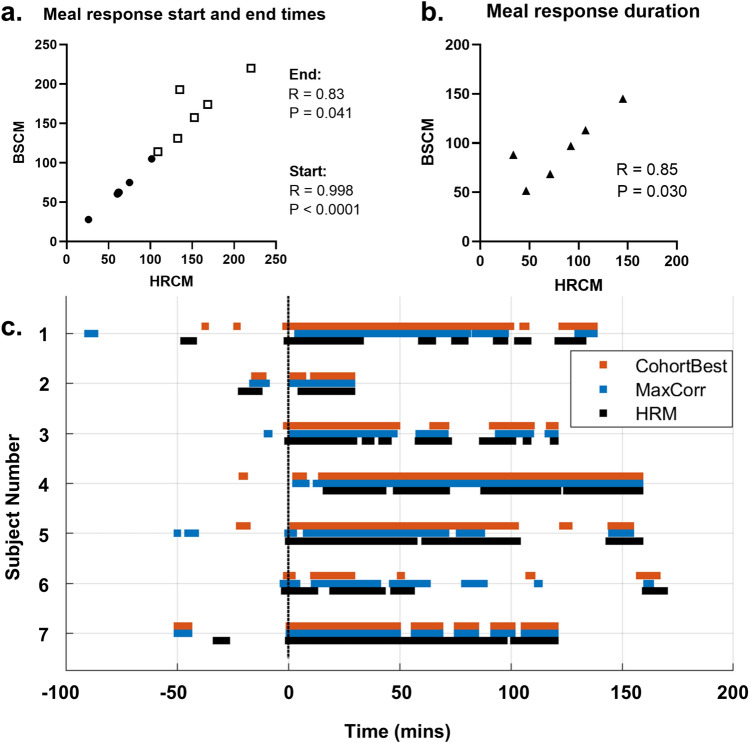
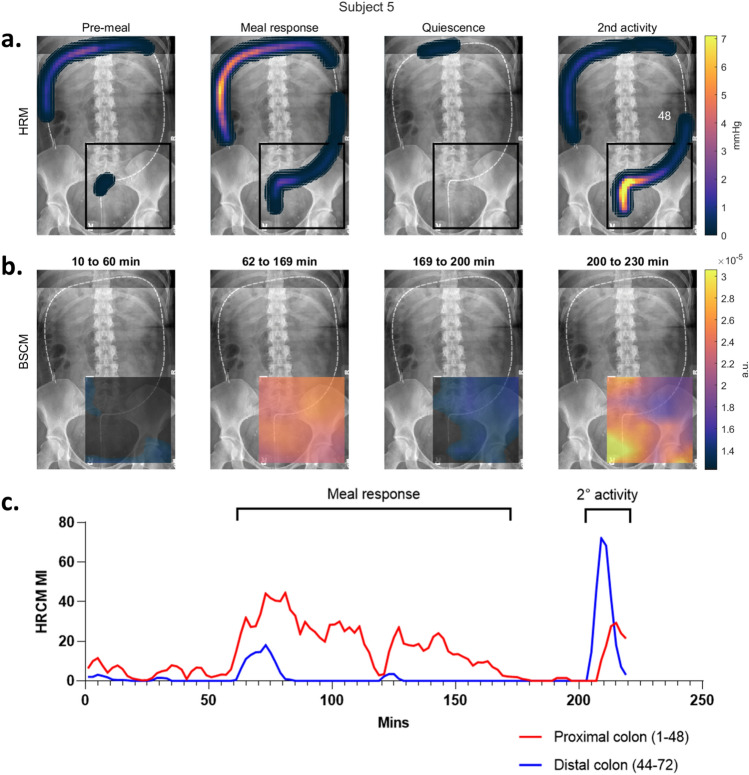
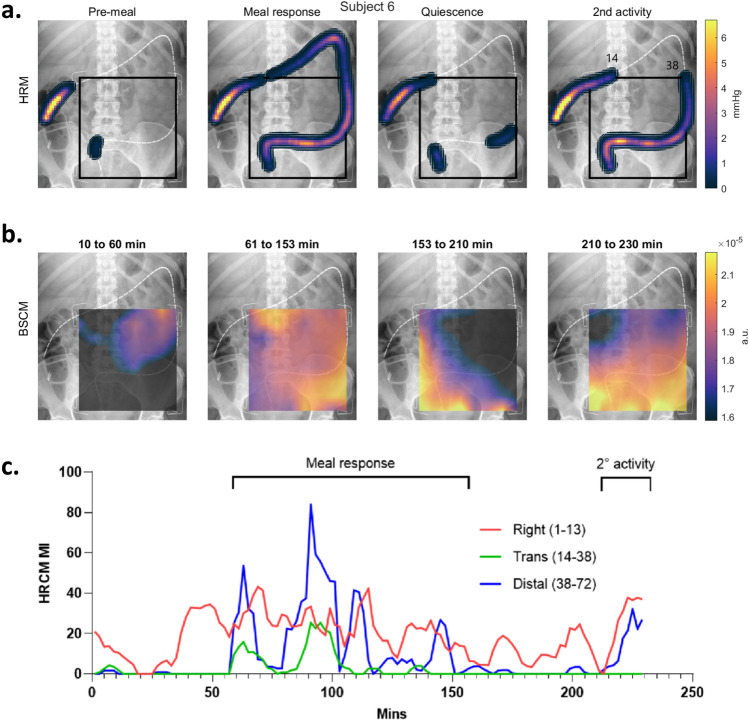
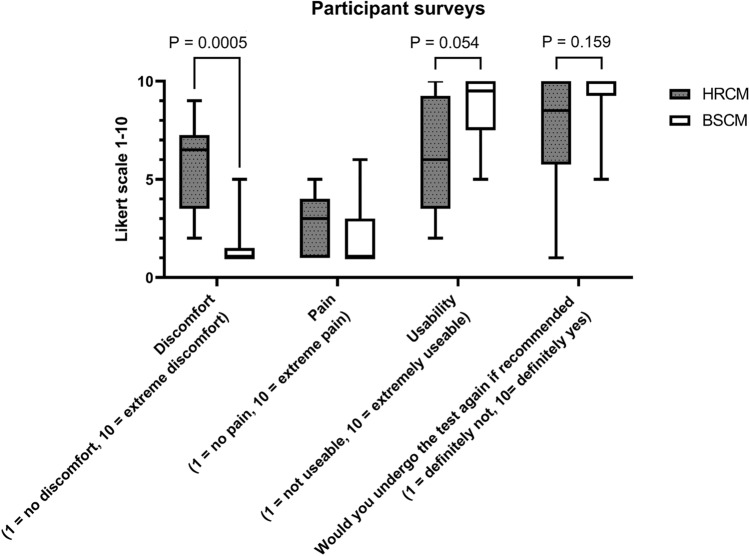
Abnormal cyclic motor pattern (CMP) activity is implicated in colonic dysfunction, but the only tool to evaluate CMP activity, high-resolution colonic manometry (HRCM), remains expensive and not widely accessible. This study aimed to validate body surface colonic mapping (BSCM) through direct correlation with HRCM. Synchronous meal-test recordings were performed in asymptomatic participants with intact colons. A signal processing method for BSCM was developed to detect CMPs. Quantitative temporal analysis was performed comparing the meal responses and motility indices (MI). Spatial heat maps were also compared. Post-study questionnaires evaluated participants' preference and comfort/distress experienced from either test. 11 participants were recruited and 7 had successful synchronous recordings (5 females/2 males; median age: 50 years [range 38-63]). The best-correlating MI temporal analyses achieved a high degree of agreement (median Pearson correlation coefficient (Rp) value: 0.69; range 0.47-0.77). HRCM and BSCM meal response start and end times (Rp = 0.998 and 0.83; both p < 0.05) and durations (Rp = 0.85; p = 0.03) were similar. Heat maps demonstrated good spatial agreement. BSCM is the first non-invasive method to be validated by demonstrating a direct spatio-temporal correlation to manometry in evaluating colonic motility.
© 2024. The Author(s).
Conflict of interest statement
This project was financially supported by CSSANZ with a Foundation Grant and HRC. Sean Ho Beom Seo is a recipient of the New Zealand Research Scholarship from RACS. Jonathan Erickson was supported by a Washington and Lee University Lenfest Sabbatical Fellowship. Greg O’Grady, Stefan Calder, Armen Gharibans and Jonathan Erickson are shareholders of Alimetry Ltd and hold intellectual property in the field of noninvasive gastric mapping. No commercial financial support was received for this study. The other authors have no conflict of interest to declare.
Figures
Similar articles
-
Use of high-resolution colonic manometry to establish etiology and direct treatment in patients with constipation: Case series with correlation to histology.J Gastroenterol Hepatol. 2018 Nov;33(11):1864-1872. doi: 10.1111/jgh.14287. Epub 2018 Jun 6. J Gastroenterol Hepatol. 2018. PMID: 29791059
-
High-resolution colonic motility recordings in vivo compared with ex vivo recordings after colectomy, in patients with slow transit constipation.Neurogastroenterol Motil. 2016 Dec;28(12):1824-1835. doi: 10.1111/nmo.12884. Epub 2016 Jun 9. Neurogastroenterol Motil. 2016. PMID: 27282132
-
High-Resolution Colonic Manometry Pressure Profiles Are Similar in Asymptomatic Diverticulosis and Controls.Dig Dis Sci. 2021 Mar;66(3):832-842. doi: 10.1007/s10620-020-06320-4. Epub 2020 May 12. Dig Dis Sci. 2021. PMID: 32399665
-
A new understanding of the physiology and pathophysiology of colonic motility?Neurogastroenterol Motil. 2018 Nov;30(11):e13395. doi: 10.1111/nmo.13395. Epub 2018 Jul 4. Neurogastroenterol Motil. 2018. PMID: 29971850 Review.
-
[Advances in colonic manometry in adults with colonic motility disorders].Zhonghua Wei Chang Wai Ke Za Zhi. 2023 Jun 25;26(6):614-617. doi: 10.3760/cma.j.cn441530-20220901-00365. Zhonghua Wei Chang Wai Ke Za Zhi. 2023. PMID: 37583017 Review. Chinese.
Cited by
-
Body Surface Gastric Mapping Delineates Specific Patient Phenotypes in Adolescents With Functional Dyspepsia and Gastroparesis.Neurogastroenterol Motil. 2025 Jun;37(6):e70018. doi: 10.1111/nmo.70018. Epub 2025 Mar 19. Neurogastroenterol Motil. 2025. PMID: 40106804 Free PMC article.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
