Control of complement-induced inflammatory responses to SARS-CoV-2 infection by anti-SARS-CoV-2 antibodies
- PMID: 38418557
- PMCID: PMC10987522
- DOI: 10.1038/s44318-024-00061-0
Control of complement-induced inflammatory responses to SARS-CoV-2 infection by anti-SARS-CoV-2 antibodies
Abstract
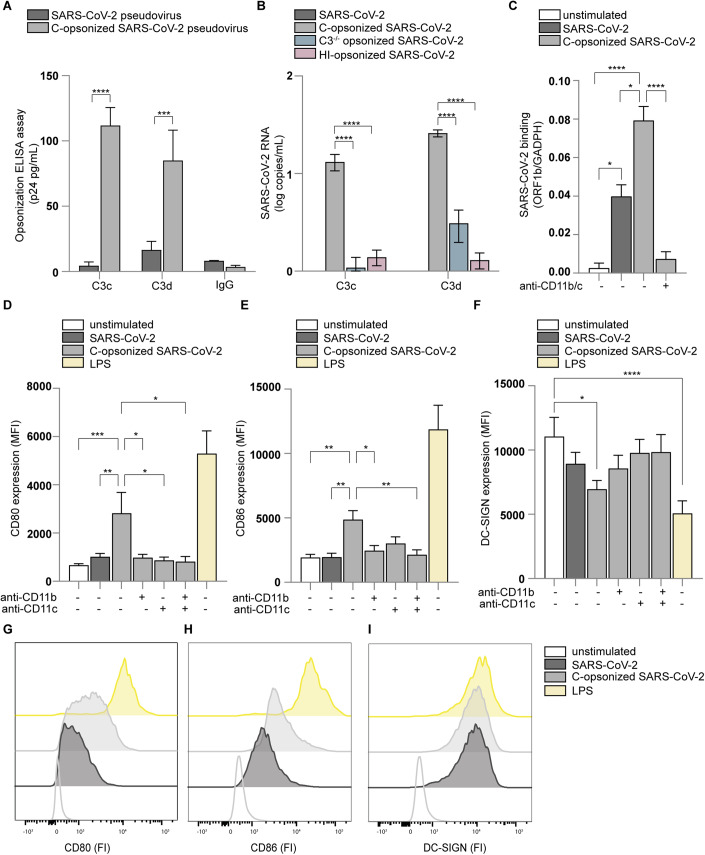
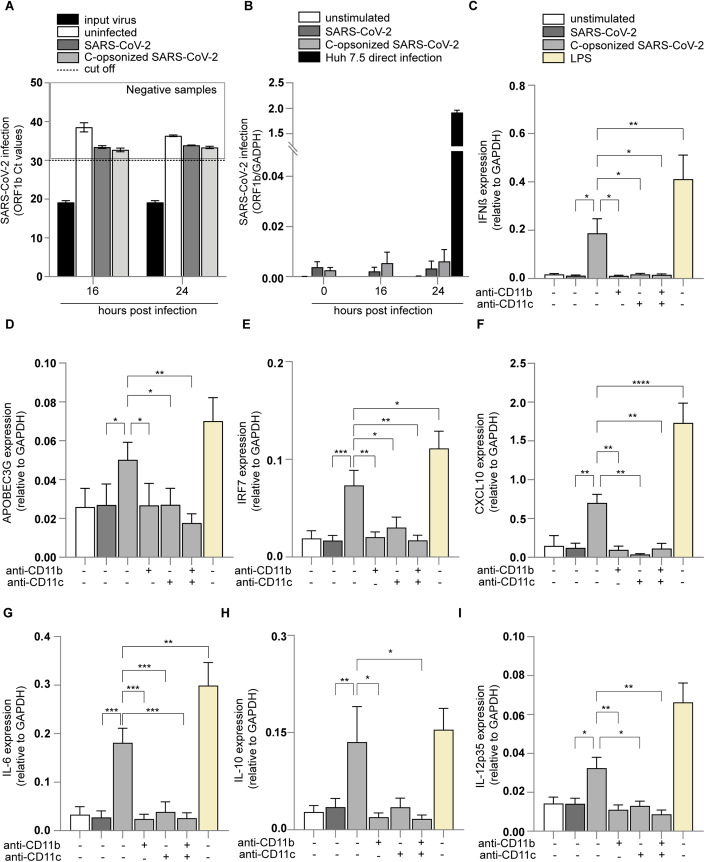
Dysregulated immune responses contribute to the excessive and uncontrolled inflammation observed in severe COVID-19. However, how immunity to SARS-CoV-2 is induced and regulated remains unclear. Here, we uncover the role of the complement system in the induction of innate and adaptive immunity to SARS-CoV-2. Complement rapidly opsonizes SARS-CoV-2 particles via the lectin pathway. Complement-opsonized SARS-CoV-2 efficiently induces type-I interferon and pro-inflammatory cytokine responses via activation of dendritic cells, which are inhibited by antibodies against the complement receptors (CR) 3 and 4. Serum from COVID-19 patients, or monoclonal antibodies against SARS-CoV-2, attenuate innate and adaptive immunity induced by complement-opsonized SARS-CoV-2. Blocking of CD32, the FcγRII antibody receptor of dendritic cells, restores complement-induced immunity. These results suggest that opsonization of SARS-CoV-2 by complement is involved in the induction of innate and adaptive immunity to SARS-CoV-2 in the acute phase of infection. Subsequent antibody responses limit inflammation and restore immune homeostasis. These findings suggest that dysregulation of the complement system and FcγRII signaling may contribute to severe COVID-19.
Keywords: COVID-19; Complement; Dendritic Cells; SARS-CoV-2; Type-I IFN Responses.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures









Similar articles
-
SARS-CoV-2 Antibodies Mediate Complement and Cellular Driven Inflammation.Front Immunol. 2021 Nov 2;12:767981. doi: 10.3389/fimmu.2021.767981. eCollection 2021. Front Immunol. 2021. PMID: 34804055 Free PMC article.
-
Lectin Pathway Mediates Complement Activation by SARS-CoV-2 Proteins.Front Immunol. 2021 Jul 5;12:714511. doi: 10.3389/fimmu.2021.714511. eCollection 2021. Front Immunol. 2021. PMID: 34290717 Free PMC article.
-
Innate and adaptive immune responses to SARS-CoV-2 in humans: relevance to acquired immunity and vaccine responses.Clin Exp Immunol. 2021 Jun;204(3):310-320. doi: 10.1111/cei.13582. Epub 2021 Mar 4. Clin Exp Immunol. 2021. PMID: 33534923 Free PMC article. Review.
-
COVID-19 Severity Is Associated with Differential Antibody Fc-Mediated Innate Immune Functions.mBio. 2021 Apr 20;12(2):e00281-21. doi: 10.1128/mBio.00281-21. mBio. 2021. PMID: 33879594 Free PMC article.
-
Complement Factors in COVID-19 Therapeutics and Vaccines.Trends Immunol. 2021 Feb;42(2):94-103. doi: 10.1016/j.it.2020.12.002. Epub 2020 Dec 13. Trends Immunol. 2021. PMID: 33402318 Free PMC article. Review.
Cited by
-
SARS-CoV-2 hijacks host CD55, CD59 and factor H to impair antibody-dependent complement-mediated lysis.Emerg Microbes Infect. 2024 Dec;13(1):2417868. doi: 10.1080/22221751.2024.2417868. Epub 2024 Oct 28. Emerg Microbes Infect. 2024. PMID: 39435487 Free PMC article.
References
-
- Bermejo-Jambrina M, Blatzer M, Jauregui-Onieva P, Yordanov TE, Hörtnagl P, Valovka T, Huber LA, Wilflingseder D, Posch W. CR4 signaling contributes to a DC-driven enhanced immune response against complement-opsonized HIV-1. Front Immunol. 2020;11:2010. doi: 10.3389/fimmu.2020.02010. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous