

Low-dose GBCA administration for brain tumour dynamic contrast enhanced MRI: a feasibility study
- PMID: 38418818
- PMCID: PMC10902320
- DOI: 10.1038/s41598-024-53871-x
Low-dose GBCA administration for brain tumour dynamic contrast enhanced MRI: a feasibility study
Abstract
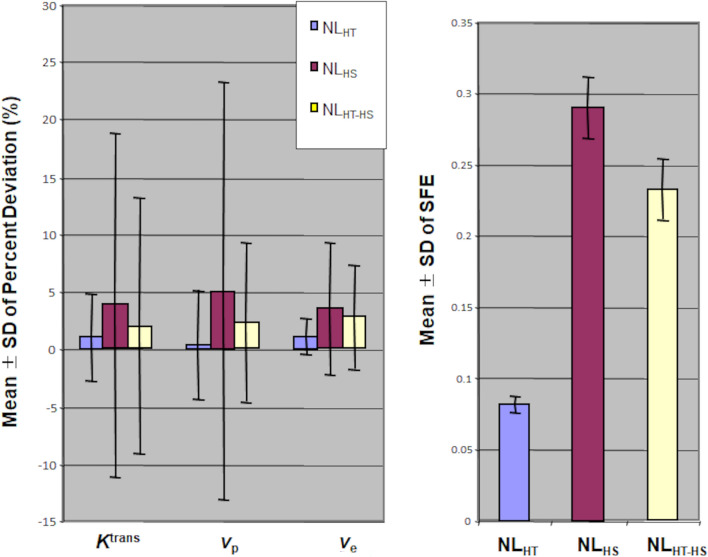
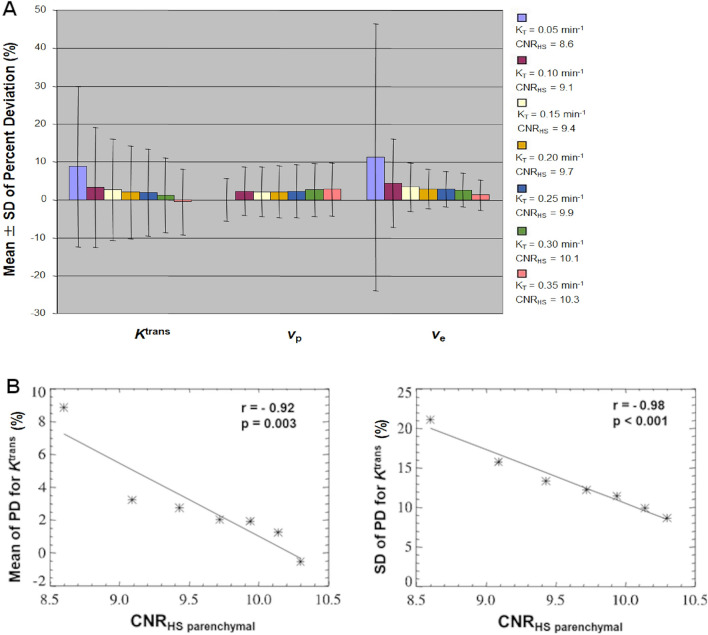
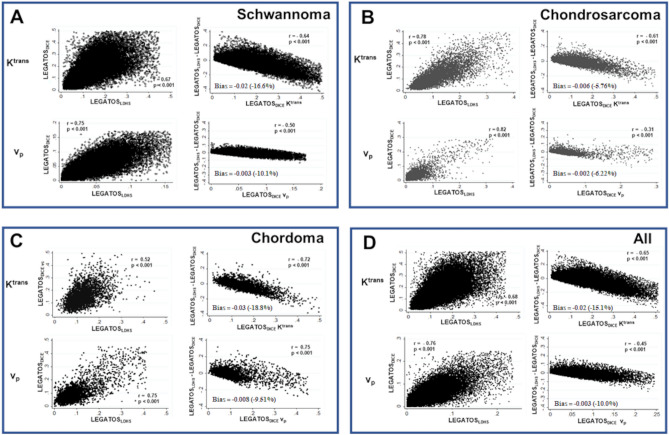
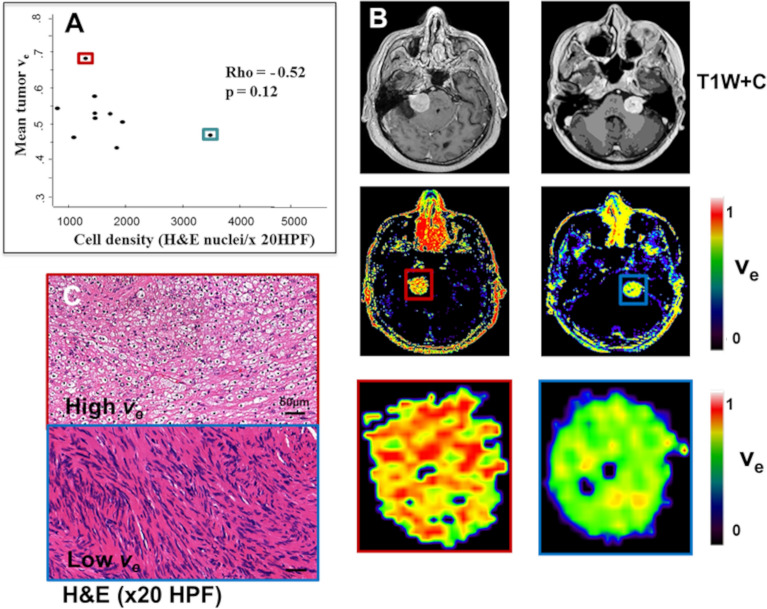
A key limitation of current dynamic contrast enhanced (DCE) MRI techniques is the requirement for full-dose gadolinium-based contrast agent (GBCA) administration. The purpose of this feasibility study was to develop and assess a new low GBCA dose protocol for deriving high-spatial resolution kinetic parameters from brain DCE-MRI. Nineteen patients with intracranial skull base tumours were prospectively imaged at 1.5 T using a single-injection, fixed-volume low GBCA dose, dual temporal resolution interleaved DCE-MRI acquisition. The accuracy of kinetic parameters (ve, Ktrans, vp) derived using this new low GBCA dose technique was evaluated through both Monte-Carlo simulations (mean percent deviation, PD, of measured from true values) and an in vivo study incorporating comparison with a conventional full-dose GBCA protocol and correlation with histopathological data. The mean PD of data from the interleaved high-temporal-high-spatial resolution approach outperformed use of high-spatial, low temporal resolution datasets alone (p < 0.0001, t-test). Kinetic parameters derived using the low-dose interleaved protocol correlated significantly with parameters derived from a full-dose acquisition (p < 0.001) and demonstrated a significant association with tissue markers of microvessel density (p < 0.05). Our results suggest accurate high-spatial resolution kinetic parameter mapping is feasible with significantly reduced GBCA dose.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures




Similar articles
-
The LEGATOS technique: A new tissue-validated dynamic contrast-enhanced MRI method for whole-brain, high-spatial resolution parametric mapping.Magn Reson Med. 2021 Oct;86(4):2122-2136. doi: 10.1002/mrm.28842. Epub 2021 May 15. Magn Reson Med. 2021. PMID: 33991126
-
Feasibility of Dynamic Contrast-Enhanced Magnetic Resonance Imaging Using Low-Dose Gadolinium: Comparative Performance With Standard Dose in Prostate Cancer Diagnosis.Invest Radiol. 2018 Oct;53(10):609-615. doi: 10.1097/RLI.0000000000000466. Invest Radiol. 2018. PMID: 29702525 Free PMC article.
-
SHILO, a novel dual imaging approach for simultaneous HI-/LOw temporal (Low-/Hi-spatial) resolution imaging for vascular dynamic contrast enhanced cardiovascular magnetic resonance: numerical simulations and feasibility in the carotid arteries.J Cardiovasc Magn Reson. 2013 May 24;15(1):42. doi: 10.1186/1532-429X-15-42. J Cardiovasc Magn Reson. 2013. PMID: 23706156 Free PMC article.
-
Surrogate vascular input function measurements from the superior sagittal sinus are repeatable and provide tissue-validated kinetic parameters in brain DCE-MRI.Sci Rep. 2022 May 24;12(1):8737. doi: 10.1038/s41598-022-12582-x. Sci Rep. 2022. PMID: 35610281 Free PMC article.
-
The role of gadolinium-based contrast agents in magnetic resonance imaging structured reporting and data systems (RADS).MAGMA. 2024 Feb;37(1):15-25. doi: 10.1007/s10334-023-01113-y. Epub 2023 Sep 13. MAGMA. 2024. PMID: 37702845 Free PMC article. Review.
Cited by
-
Role of dynamic contrast-enhanced and dynamic susceptibility contrast imaging in evaluating the biological features of glioma.Quant Imaging Med Surg. 2025 Aug 1;15(8):7030-7045. doi: 10.21037/qims-2024-2794. Epub 2025 Jul 28. Quant Imaging Med Surg. 2025. PMID: 40785876 Free PMC article.
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
