

Prediction of plasma ctDNA fraction and prognostic implications of liquid biopsy in advanced prostate cancer
- PMID: 38418825
- PMCID: PMC10902374
- DOI: 10.1038/s41467-024-45475-w
Prediction of plasma ctDNA fraction and prognostic implications of liquid biopsy in advanced prostate cancer
Abstract
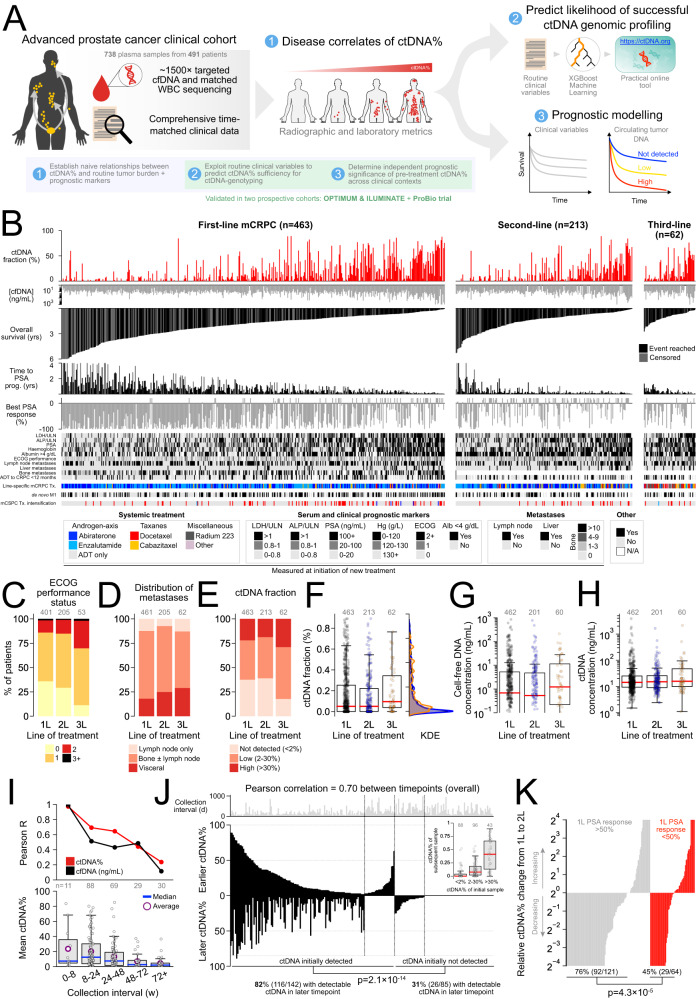
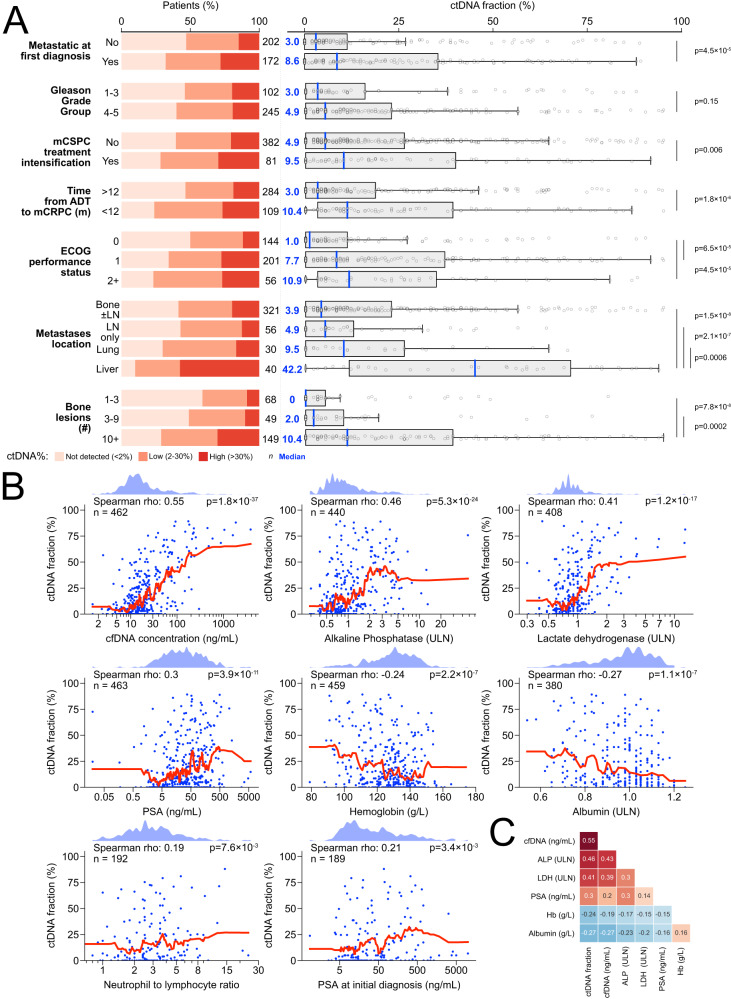
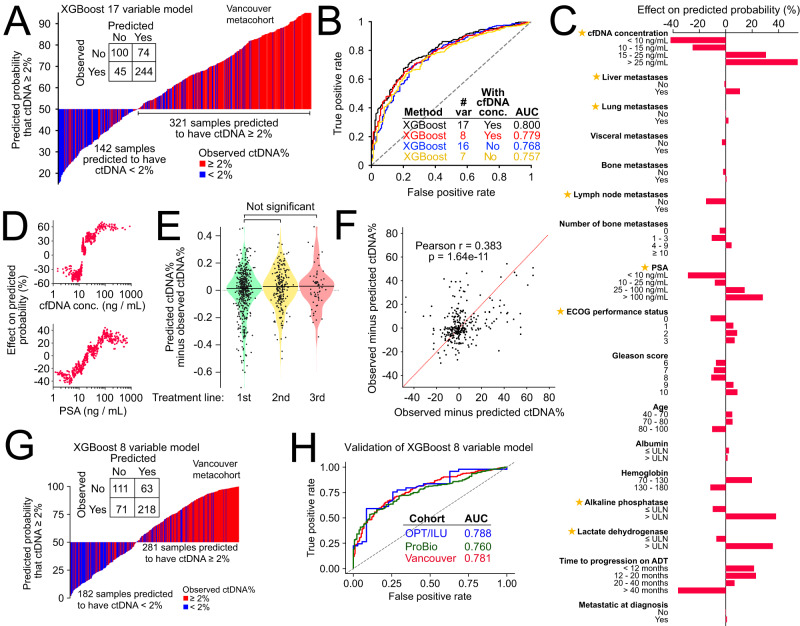
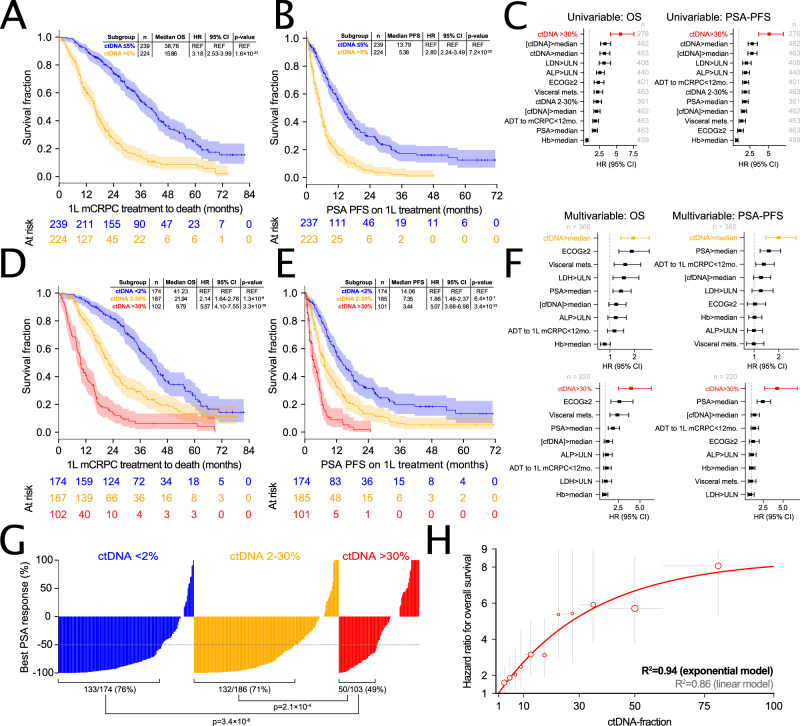
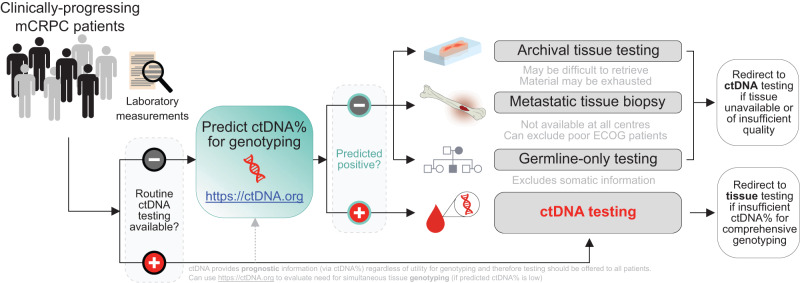
No consensus strategies exist for prognosticating metastatic castration-resistant prostate cancer (mCRPC). Circulating tumor DNA fraction (ctDNA%) is increasingly reported by commercial and laboratory tests but its utility for risk stratification is unclear. Here, we intersect ctDNA%, treatment outcomes, and clinical characteristics across 738 plasma samples from 491 male mCRPC patients from two randomized multicentre phase II trials and a prospective province-wide blood biobanking program. ctDNA% correlates with serum and radiographic metrics of disease burden and is highest in patients with liver metastases. ctDNA% strongly predicts overall survival, progression-free survival, and treatment response independent of therapeutic context and outperformed established prognostic clinical factors. Recognizing that ctDNA-based biomarker genotyping is limited by low ctDNA% in some patients, we leverage the relationship between clinical prognostic factors and ctDNA% to develop a clinically-interpretable machine-learning tool that predicts whether a patient has sufficient ctDNA% for informative ctDNA genotyping (available online: https://www.ctDNA.org ). Our results affirm ctDNA% as an actionable tool for patient risk stratification and provide a practical framework for optimized biomarker testing.
© 2024. The Author(s).
Conflict of interest statement
C.M.D. reports Honoria from MSD, Bristol-Myers Squibb, Medison and Pfizer and consulting fees from Biomica LTD. E.M.K. has served in consulting or advisory roles in Astellas Pharma, Janssen, Ipsen and received honoraria from Janssen, Ipsen, Astellas Pharma, and Research Review. E.M.K. also reports research funding from Astellas Pharma (institutional) and AstraZeneca (institutional), and travel expense reimbursement from Astellas Pharma, Pfizer, Ipsen and Roche. K.N. has served on advisory boards for Abbvie, Astellas, AstraZeneca, Bayer, Bristol-Myers Squibb, Merck, Janssen and Tersera. D.L.F. has served in advisory roles or received honorarium from Janssen, Bayer, Astellas, AstraZeneca and Pfizer. M.A. is a shareholder in Fluivia Ltd. K.N.C. reports grants from Janssen, Astellas, and Sanofi during the conduct of the study. K.N.C. also reports grants and personal fees from Janssen, Astellas, AstraZeneca, and Sanofi, as well as personal fees from Constellation Pharmaceuticals, Daiichi Sankyo, Merck, Novartis, Pfizer, Point Biopharma, and Roche outside the submitted work. A.W.W. has served on advisory boards and/or received honoraria from AstraZeneca, Astellas, Bayer, EMD Serono, Janssen, Merck, and Pfizer. A.W.W.’s laboratory has a contract research agreement with ESSA Pharma. The remaining authors declare no competing interests.
Figures
References
-
- Sung, H. et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin.71, 209–249 (2021). - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
