

Natural Killer Cell Infiltration in Prostate Cancers Predict Improved Patient Outcomes
- PMID: 38418892
- PMCID: PMC11349934
- DOI: 10.1038/s41391-024-00797-0
Natural Killer Cell Infiltration in Prostate Cancers Predict Improved Patient Outcomes
Erratum in
-
Correction: Natural killer cell infiltration in prostate cancers predict improved patient outcomes.Prostate Cancer Prostatic Dis. 2025 Dec;28(4):1030. doi: 10.1038/s41391-025-01009-z. Prostate Cancer Prostatic Dis. 2025. PMID: 40796671 Free PMC article. No abstract available.
Abstract
Background: Natural killer (NK) cells are non-antigen specific innate immune cells that can be redirected to targets of interest using multiple strategies, although none are currently FDA-approved. We sought to evaluate NK cell infiltration into tumors to develop an improved understanding of which histologies may be most amenable to NK cell-based therapies currently in the developmental pipeline.
Methods: DNA (targeted/whole-exome) and RNA (whole-transcriptome) sequencing was performed from tumors from 45 cancer types (N = 90,916 for all cancers and N = 3365 for prostate cancer) submitted to Caris Life Sciences. NK cell fractions and immune deconvolution were inferred from RNA-seq data using quanTIseq. Real-world overall survival (OS) and treatment status was determined and Kaplan-Meier estimates were calculated. Statistical significance was determined using X2 and Mann-Whitney U tests, with corrections for multiple comparisons where appropriate.
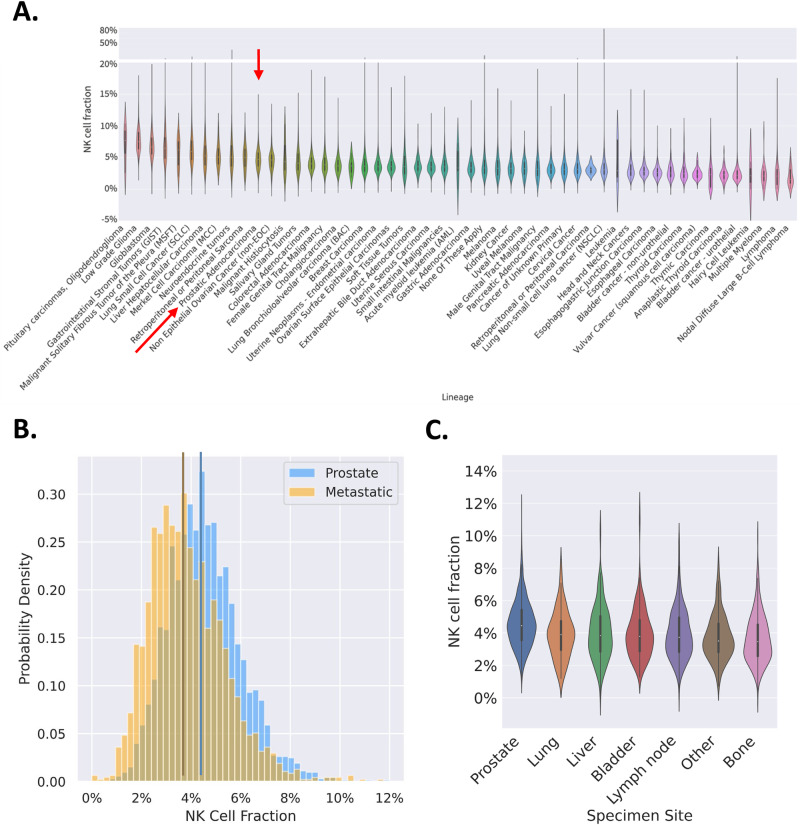
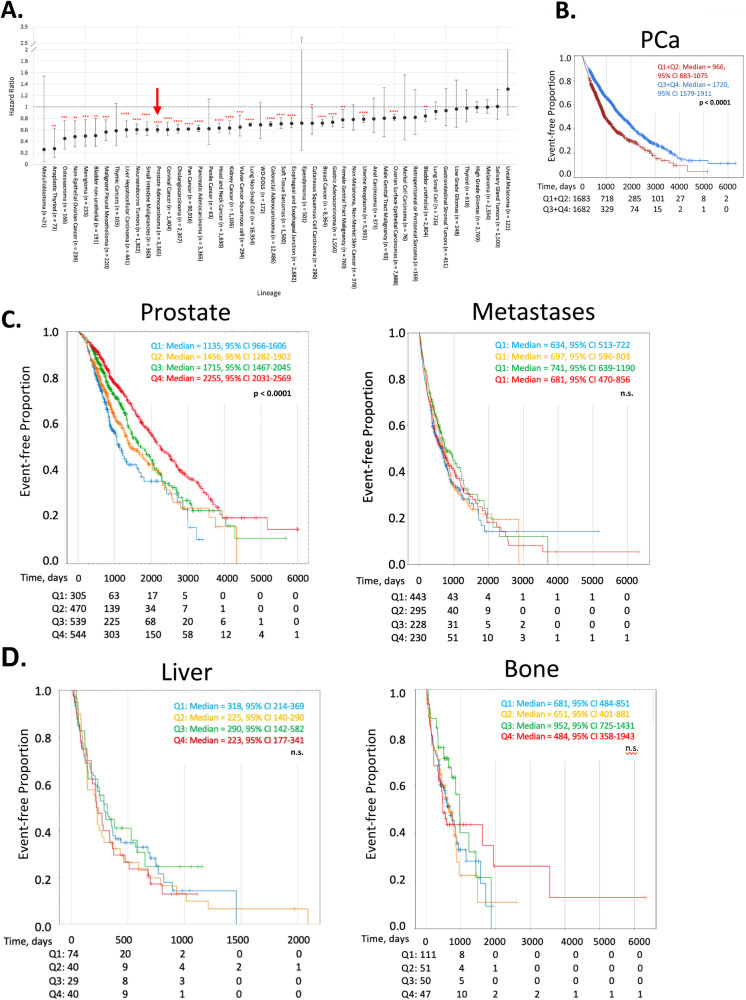
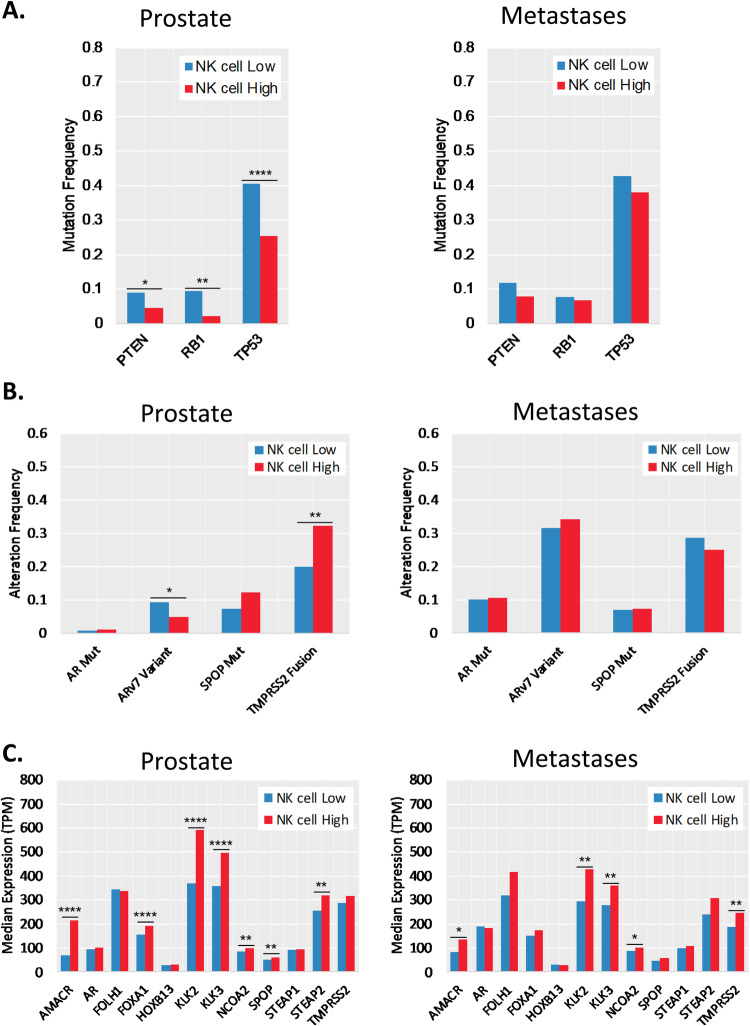
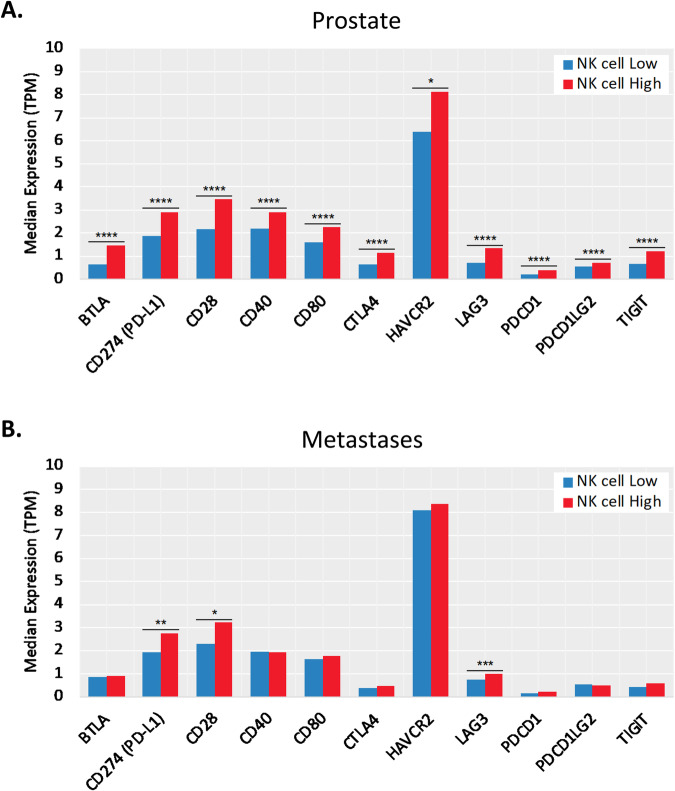
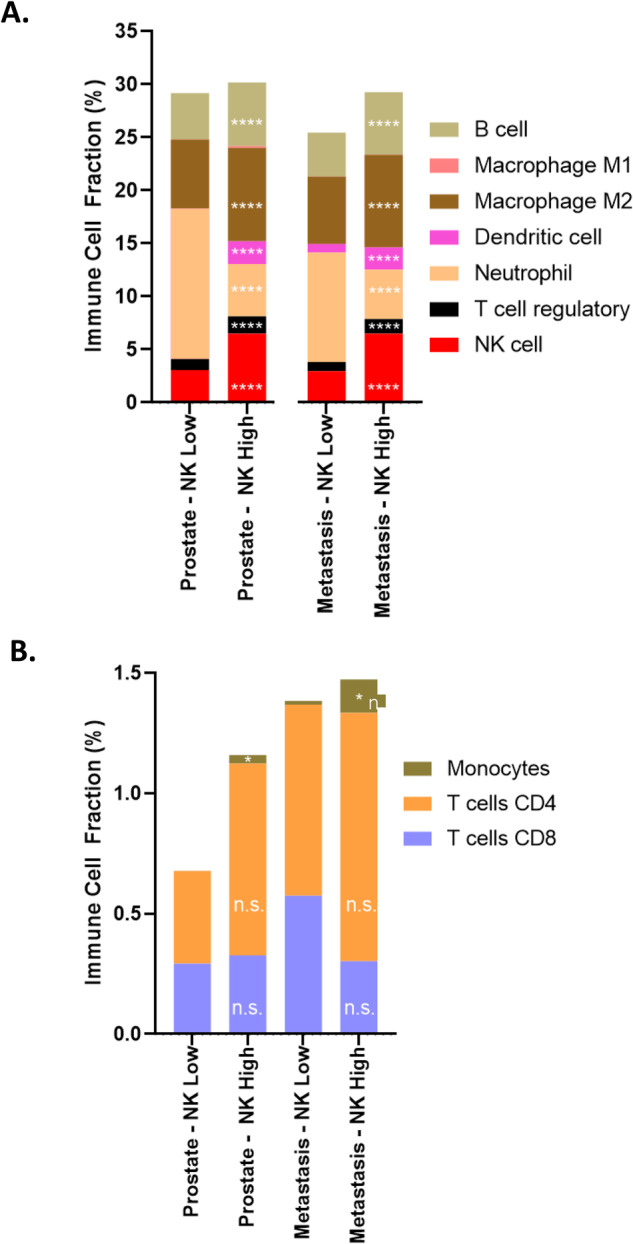
Results: In both a pan-tumor and prostate cancer (PCa) -specific setting, we demonstrated that NK cells represent a substantial proportion of the total cellular infiltrate (median range 2-9% for all tumors). Higher NK cell infiltration was associated with improved OS in 28 of 45 cancer types, including (PCa). NK cell infiltration was negatively correlated with common driver mutations and androgen receptor variants (AR-V7) in primary prostate biopsies, while positively correlated with negative immune regulators. Higher levels of NK cell infiltration were associated with patterns consistent with a compensatory anti-inflammatory response.
Conclusions: Using the largest available dataset to date, we demonstrated that NK cells infiltrate a broad range of tumors, including both primary and metastatic PCa. NK cell infiltration is associated with improved PCa patient outcomes. This study demonstrates that NK cells are capable of trafficking to both primary and metastatic PCa and are a viable option for immunotherapy approaches moving forward. Future development of strategies to enhance tumor-infiltrating NK cell-mediated cytolytic activity and activation while limiting inhibitory pathways will be key.
© 2024. The Author(s).
Conflict of interest statement
Competing interests: Nicholas Zorko reports paid travel from Caris Life Sciences and Telix Pharmaceuticals. Andrew Elliott, Milan Radovich, George Sledge, and Chadhi Nabhan are employees of Caris Life Sciences. Yousef Zakharia reports personal fees (Advisory Board) from Bristol Myers Squibb, Janssen, Eisai, Exelixis, Genzyme Corporation, Pfizer. Vivek Narayan reports grants from Janssen, Merck, Regeneron, Pfizer, and Bristol Myers Squibb; and personal fees from Janssen, Merck, Regeneron, Pfizer, Exelixis, AstraZeneca, Myovant, and Bristol Myers Squibb. Mark N. Stein serves in a consulting or advisory role for Bristol-Myers Squibb/Medarex; Exelixis; Exelixis; Janssen Oncology; Merck Sharp & Dohme; Vaccitech; Xencor and receives research funding from Advaxis (Inst); AstraZeneca (Inst); Bellicum Pharmaceuticals; Bicycle Therapeutics (Inst); Bristol-Myers Squibb (Inst); Exelixis (Inst); Genocea Biosciences (Inst); Harpoon (Inst); Janssen Oncology (Inst); Lilly (Inst); Medivation/Astellas (Inst); Merck Sharp & Dohme (Inst); Nektar (Inst); Oncoceutics (Inst); Regeneron (Inst); Seagen (Inst); Suzhou Kintor Pharmaceuticals (Inst); Tmunity Therapeutics, Inc. (Inst); Xencor (Inst). Kevin K. Zarrabi reports advising/consulting fees from Exelixis, Esai. Akash Patniak reports Consultancy/Advisory Board for Janssen, Exelixis, Jounce Therapeutics, BostonGene. Grant/Research support from BMS. Clinical Trial Support from BMS, Clovis Oncology, Progenics, Janssen, Laekna, Astrazeneca, Xencor, and Zenith. Honoraria from Exelixis, Janssen, Roche, Clovis Oncology, Merck, Prime, Curio. M.A. Bilen has acted as a paid consultant for and/or as a member of the advisory boards of Exelixis, Bayer, BMS, Eisai, Pfizer, AstraZeneca, Janssen, Calithera Biosciences, Genomic Health, Nektar, EMD Serono, SeaGen, and Sanofi and has received grants to his institution from Merck, Xencor, Bayer, Bristol-Myers Squibb, Genentech/Roche, SeaGen, Incyte, Nektar, AstraZeneca, Tricon Pharmaceuticals, Genome & Company, AAA, Peloton Therapeutics, and Pfizer for work performed as outside of the current study. Elisabeth I. Heath – Advisory/Consulting: Astellas, AstraZeneca, Bayer, Sanofi; Steering Committee: Janssen; Honararia/Paid Travel: Astellas, Bayer, Caris, Sanofi, Seattle Genetics; Speaker’s Bureau: Sanofi; Research Support: Astellas, Arvinas, AstraZeneca, Bayer, BioXcel, Bristol-Myers Squibb, Calibr, Calithera, Caris, Corcept, Corvis, Daiichi Sankyo, Eisai, Exelixis, Five Prime, Fortis, GlaxoSmithKline, Gilead Sciences, Harpoon, Hoffman-La Roche, Infinity, iTeos, Janssen, Merck Sharp & Dohme, Merck, Mirati, Modra, Novartis, Oncolys, Peloton, Pfizer, Pharmacyclics, POINT Biopharma, Seattle Genetics. Emmanuel S. Antonarakis reports grants and personal fees from Janssen, Sanofi, Bayer, Bristol Myers Squibb, Curium, Novartis, Merck, Pfizer, AstraZeneca, Clovis, and Orion; and personal fees from Astellas, Amgen, Blue Earth, Exact Sciences, Invitae, Eli Lilly, and Foundation Medicine; in addition, he has an issued patent for an AR-V7 biomarker technology that is licensed to Qiagen. The remaining authors have no relevant discolsures or conflicts of interest to declare.
Figures
References
-
- Antonarakis ES, Park SH, Goh JC, Shin SJ, Lee JL, Mehra N, et al. Pembrolizumab plus olaparib for patients with previously treated and biomarker-unselected metastatic castration-resistant prostate cancer: the randomized, open-label, phase III KEYLYNK-010 trial. J Clin Oncol. 2023;41:3839. - PMC - PubMed
-
- Kantoff PW, Higano CS, Shore ND, Berger ER, Small EJ, Penson DF, et al. Sipuleucel-T immunotherapy for castration-resistant prostate cancer. N. Engl J Med. 2010;363:411–22. - PubMed
-
- Hansen A, Massard C, Ott P, Haas N, Lopez J, Ejadi S, et al. Pembrolizumab for advanced prostate adenocarcinoma: findings of the KEYNOTE-028 study. Ann Oncol. 2018;29:1807–13. - PubMed
MeSH terms
Substances
Grants and funding
- W81XWH2110255/U.S. Department of Defense (United States Department of Defense)
- R35 CA283892/CA/NCI NIH HHS/United States
- P30 CA077598/CA/NCI NIH HHS/United States
- P01 CA065493/CA/NCI NIH HHS/United States
- W81XWH-21-1-0255/U.S. Department of Defense (United States Department of Defense)
- Medical Student Minority Award/American Society of Hematology (ASH)
- R01 HL122216/HL/NHLBI NIH HHS/United States
- 22YOUN08/Prostate Cancer Foundation (PCF)
- R35 CA197292/CA/NCI NIH HHS/United States
- W81XWH-20-1-0341/U.S. Department of Defense (United States Department of Defense)
- P01 CA111412/CA/NCI NIH HHS/United States
- T32 GM008244/GM/NIGMS NIH HHS/United States
- W81XWH-20-1-0535/U.S. Department of Defense (United States Department of Defense)
- R01 CA273914/CA/NCI NIH HHS/United States
- W81XWH-22-1-0242/U.S. Department of Defense (United States Department of Defense)
- W81XWH-20-1-0659/U.S. Department of Defense (United States Department of Defense)
LinkOut - more resources
Full Text Sources
Medical
Research Materials
