

Trends in low-value GP care during the COVID-19 pandemic: a retrospective cohort study
- PMID: 38418951
- PMCID: PMC10900726
- DOI: 10.1186/s12875-024-02306-7
Trends in low-value GP care during the COVID-19 pandemic: a retrospective cohort study
Erratum in
-
Correction: Trends in low-value GP care during the COVID-19 pandemic: a retrospective cohort study.BMC Prim Care. 2024 Nov 26;25(1):403. doi: 10.1186/s12875-024-02652-6. BMC Prim Care. 2024. PMID: 39592956 Free PMC article. No abstract available.
Abstract
Background: Several studies showed that during the pandemic patients have refrained from visiting their general practitioner (GP). This resulted in medical care being delayed, postponed or completely forgone. The provision of low-value care, i.e. care which offers no net benefit for the patient, also could have been affected. We therefore assessed the impact of the COVID-19 restrictions on three types of low-value GP care: 1) imaging for back or knee problems, 2) antibiotics for otitis media acuta (OMA), and 3) repeated opioid prescriptions, without a prior GP visit.
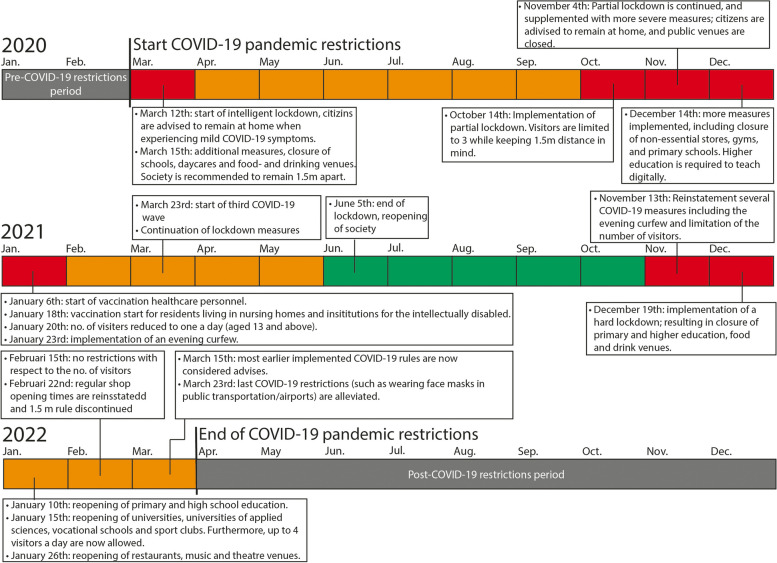
Methods: We performed a retrospective cohort study using registration data from GPs part of an academic GP network over the period 2017-2022. The COVID-19 period was defined as the period between April 2020 to December 2021. The periods before (January 2017 to April 2020) and after the COVID-19 period (January 2022 to December 2022) are the pre- and post-restrictions periods. The three clinical practices examined were selected by two practicing GPs from a top 30 of recommendations originating from the Dutch GP guidelines, based on their perceived prevalence and relevance in practice (van Dulmen et al., BMC Primary Care 23:141, 2022). Multilevel Poisson regression models were built to examine changes in the incidence rates (IR) of both registered episodes and episodes receiving low-value treatment.
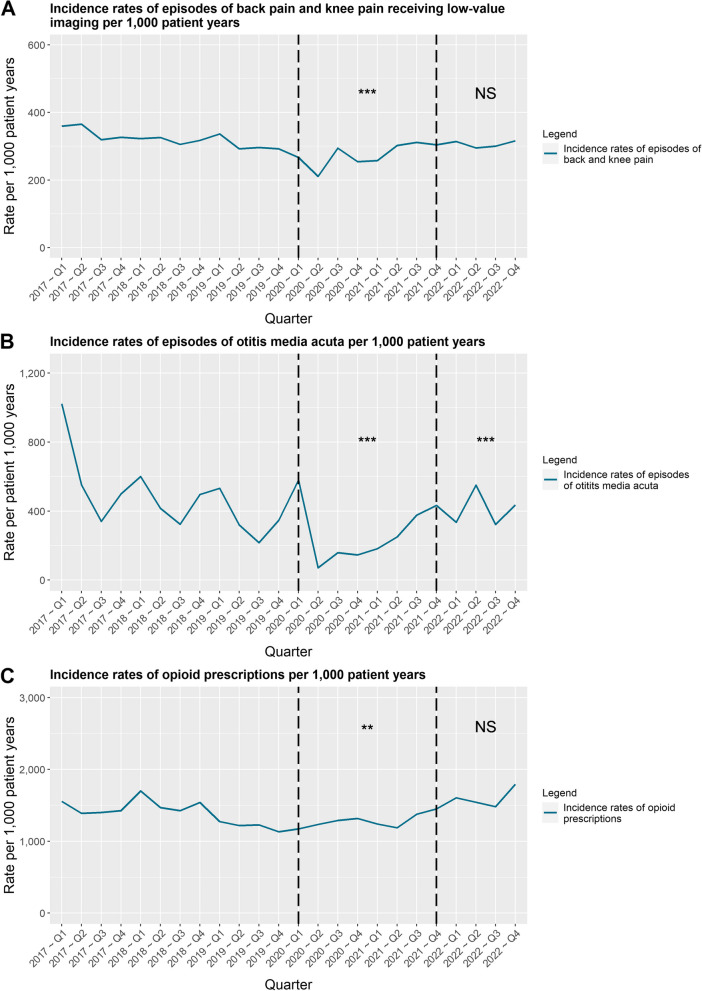
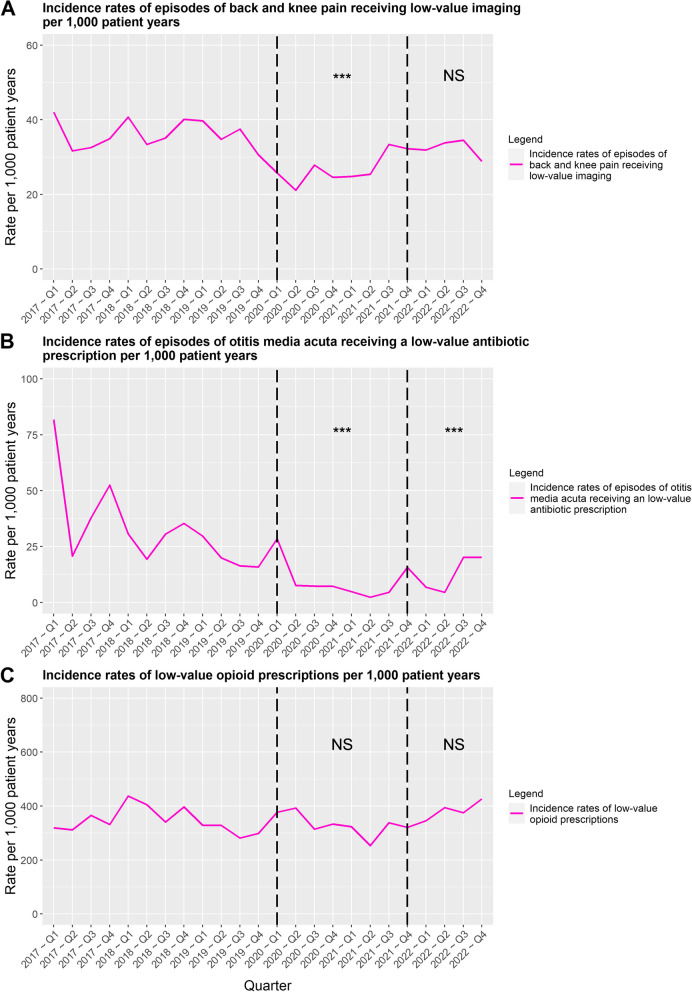
Results: During the COVID-19 restrictions period, the IRs of episodes of all three types of GP care decreased significantly. The IR of episodes of back or knee pain decreased by 12%, OMA episodes by 54% and opioid prescription rate by 13%. Only the IR of OMA episodes remained significantly lower (22%) during the post-restrictions period. The provision of low-value care also changed. The IR of imaging for back or knee pain and low-value prescription of antibiotics for OMA both decreased significantly during the COVID-restrictions period (by 21% and 78%), but only the low-value prescription rate of antibiotics for OMA remained significantly lower (by 63%) during the post-restrictions period. The IR of inappropriately repeated opioid prescriptions remained unchanged over all three periods.
Conclusions: This study shows that both the rate of episodes as well as the rate at which low-value care was provided have generally been affected by the COVID-19 restrictions. Furthermore, it shows that the magnitude of the impact of the restrictions varies depending on the type of low-value care. This indicates that deimplementation of low-value care requires tailored (multiple) interventions and may not be achieved through a single disruption or intervention alone.
Keywords: COVID-19; General practice; Low-value care; Quality of Health Care.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- World Health Organization (WHO). Public Health and Social Measures in Response to COVID-19: World Health Organization (WHO),; 2023 [updated 09–03–2023. Available from: https://phsm.euro.who.int/.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous