

Dormancy of cutaneous melanoma
- PMID: 38419052
- PMCID: PMC10903048
- DOI: 10.1186/s12935-024-03278-5
Dormancy of cutaneous melanoma
Abstract
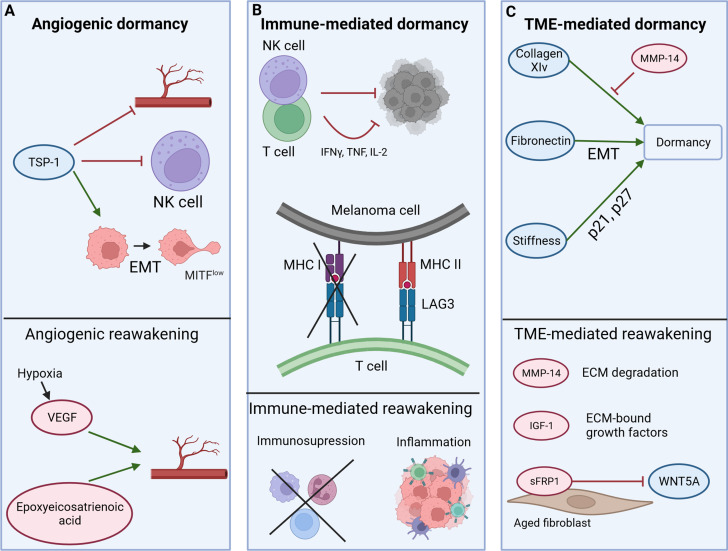
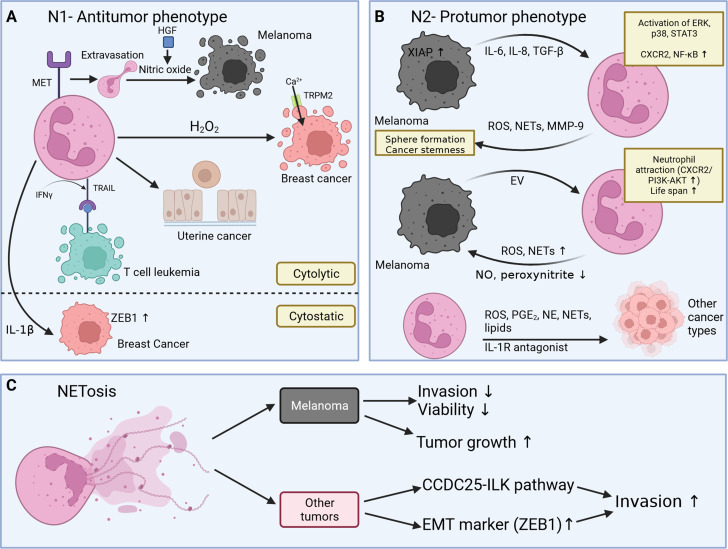
Many cancer-related deaths including melanoma result from metastases that develop months or years after the initial cancer therapy. Even the most effective drugs and immune therapies rarely eradicate all tumor cells. Instead, they strongly reduce cancer burden, permitting dormant cancer cells to persist in niches, where they establish a cellular homeostasis with their host without causing clinical symptoms. Dormant cancers respond poorly to most drugs and therapies since they do not proliferate and hide in niches. It therefore remains a major challenge to develop novel therapies for dormant cancers. In this review we focus on the mechanisms regulating the initiation of cutaneous melanoma dormancy as well as those which are involved in reawakening of dormant cutaneous melanoma cells. In recent years the role of neutrophils and niche components in reawakening of melanoma cells came into focus and indicate possible future therapeutic applications. Sophisticated in vitro and in vivo melanoma dormancy models are needed to make progress in this field and are discussed.
Keywords: Dormant cancer; Immunotherapy; Melanoma; NETs; Neutrophils.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interest.
Figures

Similar articles
-
The Genetic Basis of Dormancy and Awakening in Cutaneous Metastatic Melanoma.Cancers (Basel). 2022 Apr 23;14(9):2104. doi: 10.3390/cancers14092104. Cancers (Basel). 2022. PMID: 35565234 Free PMC article. Review.
-
The Role of the Innate Immune System in Cancer Dormancy and Relapse.Cancers (Basel). 2021 Nov 10;13(22):5621. doi: 10.3390/cancers13225621. Cancers (Basel). 2021. PMID: 34830776 Free PMC article. Review.
-
Tuning Cancer Fate: Tumor Microenvironment's Role in Cancer Stem Cell Quiescence and Reawakening.Front Immunol. 2020 Oct 21;11:2166. doi: 10.3389/fimmu.2020.02166. eCollection 2020. Front Immunol. 2020. PMID: 33193295 Free PMC article. Review.
-
Immunogenic, cellular, and angiogenic drivers of tumor dormancy--a melanoma view.Pigment Cell Melanoma Res. 2016 Jan;29(1):27-42. doi: 10.1111/pcmr.12432. Epub 2015 Nov 27. Pigment Cell Melanoma Res. 2016. PMID: 26514653 Review.
-
Dormancy in breast cancer.Breast Cancer (Dove Med Press). 2012 Dec 5;4:183-91. doi: 10.2147/BCTT.S26431. Breast Cancer (Dove Med Press). 2012. PMID: 24367205 Free PMC article. Review.
Cited by
-
Modeling a mesenchymal cell state by bioprinting for the molecular analysis of dormancy in melanoma.Mater Today Bio. 2025 Mar 18;32:101674. doi: 10.1016/j.mtbio.2025.101674. eCollection 2025 Jun. Mater Today Bio. 2025. PMID: 40206148 Free PMC article.
-
Minimal residual disease as a target for liquid biopsy in patients with solid tumours.Nat Rev Clin Oncol. 2025 Jan;22(1):65-77. doi: 10.1038/s41571-024-00967-y. Epub 2024 Nov 28. Nat Rev Clin Oncol. 2025. PMID: 39609625 Review.
-
Skin Malignant Melanoma and Matrix Metalloproteinases: Promising Links to Efficient Therapies.Int J Mol Sci. 2024 Jul 17;25(14):7804. doi: 10.3390/ijms25147804. Int J Mol Sci. 2024. PMID: 39063046 Free PMC article. Review.
-
Correctly identifying the cells of origin is essential for tailoring treatment and understanding the emergence of cancer stem cells and late metastases.Front Oncol. 2024 Apr 10;14:1369907. doi: 10.3389/fonc.2024.1369907. eCollection 2024. Front Oncol. 2024. PMID: 38660133 Free PMC article. Review.
-
Tumor dormancy and relapse: understanding the molecular mechanisms of cancer recurrence.Mil Med Res. 2025 Feb 11;12(1):7. doi: 10.1186/s40779-025-00595-2. Mil Med Res. 2025. PMID: 39934876 Free PMC article. Review.
References
-
- Robert Koch-Institut. (2021). Krebs in Deutschland für 2017/2018. 72–74, 10.25646/8353.
-
- Eggermont AMM, Chiarion-Sileni V, Grob J-J, Dummer R, Wolchok JD, Schmidt H, et al. Adjuvant ipilimumab versus placebo after complete resection of high-risk stage III melanoma (EORTC 18071): a randomised, double-blind, phase 3 trial. Lancet Oncol. 2015;16(5):522–30. doi: 10.1016/S1470-2045(15)70122-1. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
