

Dietary intake and gastrointestinal symptoms are altered in children with Autism Spectrum Disorder: the relative contribution of autism-linked traits
- PMID: 38419087
- PMCID: PMC10900601
- DOI: 10.1186/s12937-024-00930-8
Dietary intake and gastrointestinal symptoms are altered in children with Autism Spectrum Disorder: the relative contribution of autism-linked traits
Erratum in
-
Correction: Dietary intake and gastrointestinal symptoms are altered in children with Autism Spectrum Disorder: the relative contribution of autism-linked traits.Nutr J. 2024 Apr 2;23(1):40. doi: 10.1186/s12937-024-00942-4. Nutr J. 2024. PMID: 38566135 Free PMC article. No abstract available.
Abstract
Background: Dietary and gastrointestinal (GI) problems have been frequently reported in autism spectrum disorder (ASD). However, the relative contributions of autism-linked traits to dietary and GI problems in children with ASD are poorly understood. This study firstly compared the dietary intake and GI symptoms between children with ASD and typically developing children (TDC), and then quantified the relative contributions of autism-linked traits to dietary intake, and relative contributions of autism-linked traits and dietary intake to GI symptoms within the ASD group.
Methods: A sample of 121 children with ASD and 121 age-matched TDC were eligible for this study. The dietary intake indicators included food groups intakes, food variety, and diet quality. The autism-linked traits included ASD symptom severity, restricted repetitive behaviors (RRBs), sensory profiles, mealtime behaviors, and their subtypes. Linear mixed-effects models and mixed-effects logistic regression models were used to estimate the relative contributions.
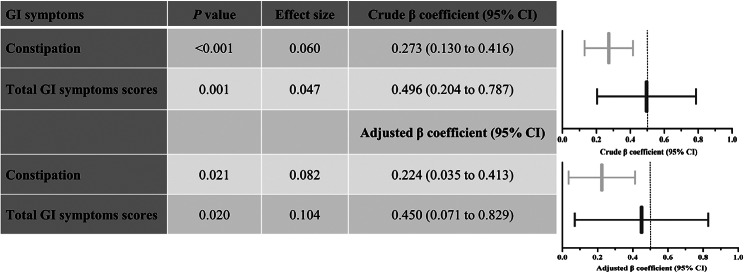
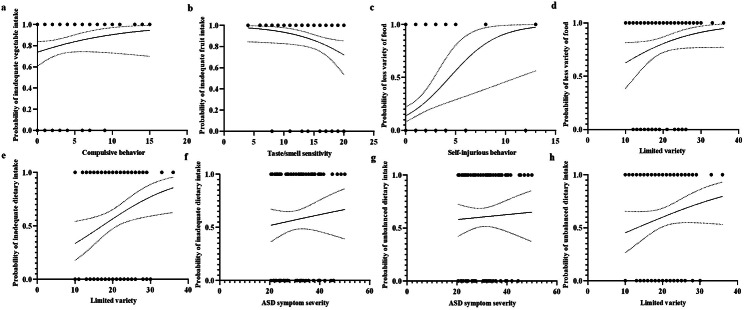
Results: Children with ASD had poorer diets with fewer vegetables/fruits, less variety of food, a higher degree of inadequate/unbalanced dietary intake, and more severe constipation/total GI symptoms than age-matched TDC. Within the ASD group, compulsive behavior (a subtype of RRBs) and taste/smell sensitivity were the only traits associated with lower vegetables and fruit consumption, respectively. Self-injurious behavior (a subtype of RRBs) was the only contributing trait to less variety of food. Limited variety (a subtype of mealtime behavior problems) and ASD symptom severity were the primary and secondary contributors to inadequate dietary intake, respectively. ASD symptom severity and limited variety were the primary and secondary contributors to unbalanced dietary intake, respectively. Notably, unbalanced dietary intake was a significant independent factor associated with constipation/total GI symptoms, and autism-linked traits manifested no contributions.
Conclusions: ASD symptom severity and unbalanced diets were the most important contributors to unbalanced dietary intake and GI symptoms, respectively. Our findings highlight that ASD symptom severity and unbalanced diets could provide the largest benefits for the dietary and GI problems of ASD if they were targeted for early detection and optimal treatment.
Keywords: Autism spectrum disorder; Autism-linked traits; Dietary intake; Gastrointestinal symptoms; Relative contributions.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



References
-
- Bi XS, Fan XZ, Mi WL, He HZ. A comparison of diagnostic criteria on the autism spectrum disorder observation for ICD-11 and DSM-5. J Int Psychiatry. 2021;48:193–6.
-
- Genovese A, Ellerbeck K. Autism spectrum disorder: a review of behavioral and psychiatric challenges across the lifespan. SN Compr Clin Med. 2022;4:217. doi: 10.1007/s42399-022-01302-1. - DOI
MeSH terms
Grants and funding
- 2019B030335001/Key-Area Research and Development Program of Guangdong Province
- K19-51000-052/Research Program of Guangzhou Disabled Persons' Federation
- 81872639/National Natural Science Foundation of China
- 2021A1515010439/Guangdong Provincial Natural Science Foundation
- 2120001008276/Social-Area Science and Technology Research Program of Foshan City
LinkOut - more resources
Full Text Sources
Medical
