

Epidemiology and clinical features of SARS-CoV-2 infection in children and adolescents in the pre-Omicron era: A global systematic review and meta-analysis
- PMID: 38419461
- PMCID: PMC10902805
- DOI: 10.7189/jogh.14.05003
Epidemiology and clinical features of SARS-CoV-2 infection in children and adolescents in the pre-Omicron era: A global systematic review and meta-analysis
Abstract
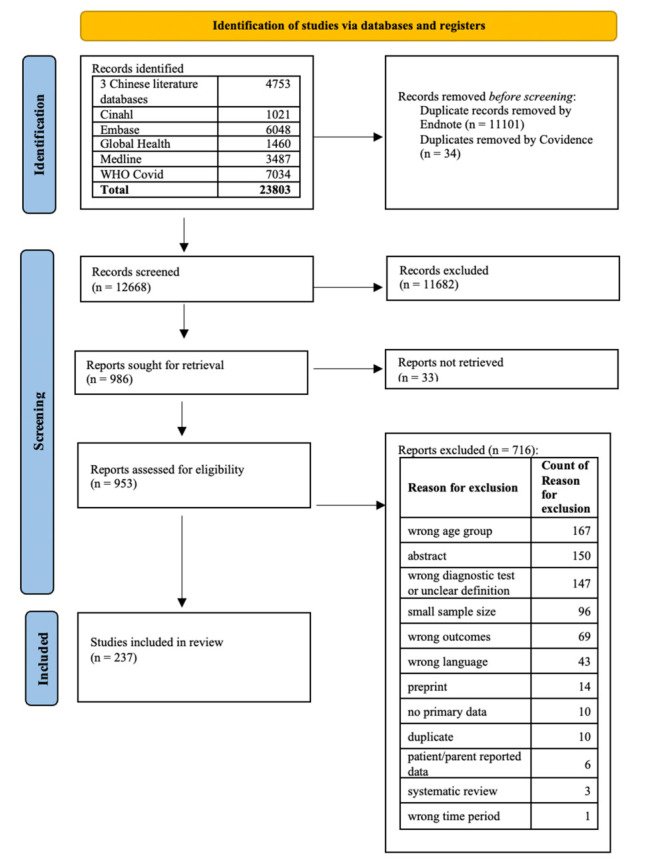
Methods: We searched MEDLINE, Embase, Global Health, CINAHL, China National Knowledge Infrastructure, Wanfang, CQvip, and the World Health Organization (WHO) COVID-19 global literature databases for primary studies recruiting children aged ≤18 years with a diagnosis of SARS-CoV-2 infection confirmed either by molecular or antigen tests. We used the Joanna Briggs Institute critical appraisal tools to appraise the study quality and conducted meta-analyses using the random effects model for all outcomes except for race/ethnicity as risk factors of SARS-CoV-2 infection.
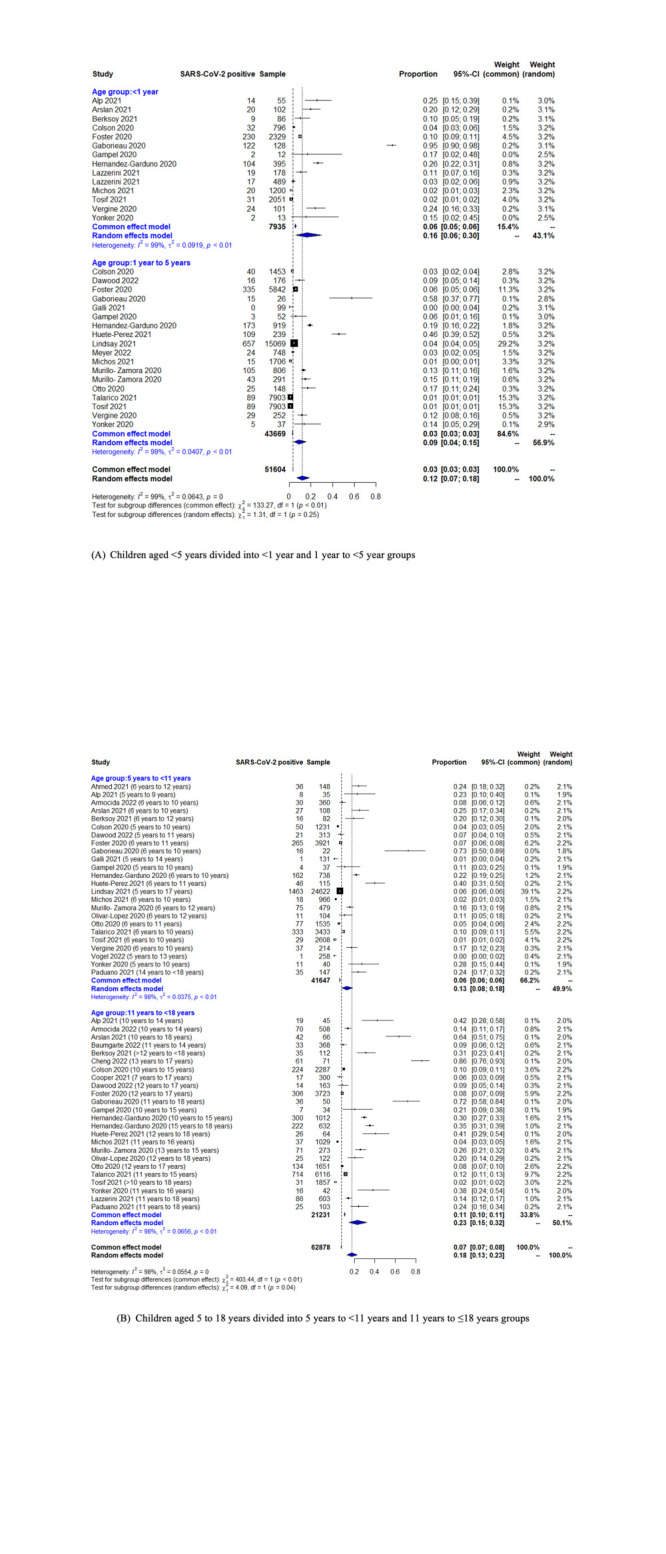
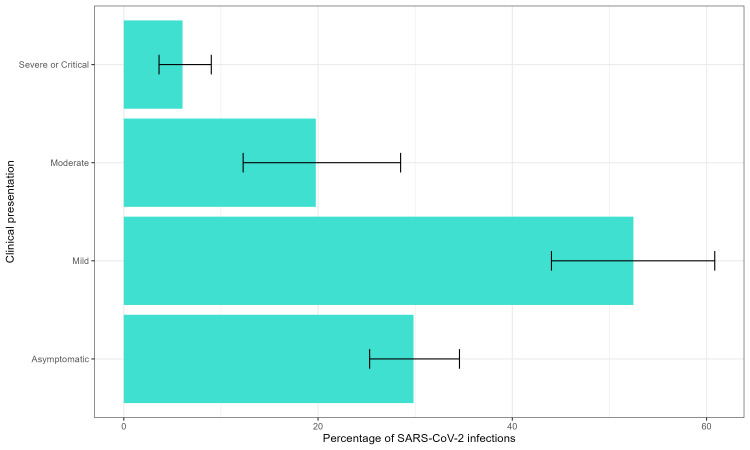
Results: We included 237 studies, each reporting at least one of the study outcomes. Based on data from 117 studies, the pooled SARS-CoV-2 positivity rate was 9.30% (95% confidence interval (CI) = 7.15-11.73). Having a comorbidity was identified as a risk factor for SARS-CoV-2 infection (risk ratio (RR) = 1.33; 95% CI = 1.04-1.71) based on data from 49 studies. Most cases in this review presented with mild disease (n = 50; 52.47% (95% CI = 44.03-60.84)). However, 20.70% of paediatric SARS-CoV-2 infections were hospitalised (67 studies), 7.19% required oxygen support (57 studies), 4.26% required intensive care (93 studies), and 2.92% required assisted ventilation (63 studies). The case fatality ratio (n = 119) was 0.87% (95% CI = 0.54-1.28), which included in-hospital and out-of-hospital deaths.
Conclusions: Our data showed that children were at risk for SARS-CoV-2 infections and severe outcomes in the pre-Omicron era. These findings underscore the need for effective vaccination strategies for the paediatric population to protect against the acute and long-term sequelae of COVID-19.
Registration: PROSPERO: CRD42022327680.
Copyright © 2024 by the Journal of Global Health. All rights reserved.
Conflict of interest statement
Disclosure of interest: The authors completed the ICMJE Disclosure of Interest Form (available upon request from the corresponding author) and disclose the following activities and/or relationships: DK reports consulting fees from Pfizer, related to the submitted work and outside the submitted work. XW received research grants from GlaxoSmithKline, Wellcome Trust, and Nanjing Medical University, outside the submitted work, and consultancy fees from Pfizer, related to the submitted work. AS, JS, and MHK are employees of Pfizer. AS was a Pfizer employee during study conduct and manuscript development and may hold stock options; he is currently employed by Orbital Therapeutics. HN reports consulting fees from Pfizer, related to the submitted work; and grants from the Innovative Medicines Initiative outside the submitted work; consulting fees from the Gates Foundation, Pfizer, and Sanofi; honoraria from AbbVie; support from Sanofi for attending meetings; and participation on advisory boards from GSK, Merck, Pfizer, Sanofi, Icosavax, Janssen, Novavax, Reviral, Resvinet, and WHO outside the submitted work.
Figures
Similar articles
-
Incidence and outcome of SARS-CoV-2 reinfection in the pre-Omicron era: A global systematic review and meta-analysis.J Glob Health. 2023 Nov 24;13:06051. doi: 10.7189/jogh.13.06051. J Glob Health. 2023. PMID: 37994839 Free PMC article.
-
Incidence, severity, risk factors and outcomes of SARS-CoV-2 reinfections during the Omicron period: a systematic review and meta-analysis.J Glob Health. 2025 Feb 7;15:04032. doi: 10.7189/jogh.15.04032. J Glob Health. 2025. PMID: 39916552 Free PMC article.
-
New-onset type 1 diabetes in children and adolescents as postacute sequelae of SARS-CoV-2 infection: A systematic review and meta-analysis of cohort studies.J Med Virol. 2023 Jun;95(6):e28833. doi: 10.1002/jmv.28833. J Med Virol. 2023. PMID: 37264687
-
The effect of COVID-19 vaccine to the Omicron variant in children and adolescents: a systematic review and meta-analysis.Front Public Health. 2024 Apr 10;12:1338208. doi: 10.3389/fpubh.2024.1338208. eCollection 2024. Front Public Health. 2024. PMID: 38660347 Free PMC article.
-
COVID-19 infection in children with blood cancer: A systematic review.Ann Hematol. 2025 Feb;104(2):1203-1230. doi: 10.1007/s00277-024-06057-4. Epub 2024 Nov 5. Ann Hematol. 2025. PMID: 39496811 Free PMC article.
Cited by
-
Characteristics and outcomes in severe and critically ill children with first wave SARS-CoV-2 Omicron infection in Northeast China.Front Cell Infect Microbiol. 2025 Apr 15;15:1495783. doi: 10.3389/fcimb.2025.1495783. eCollection 2025. Front Cell Infect Microbiol. 2025. PMID: 40302919 Free PMC article.
-
The Improvement of Adaptive Immune Responses towards COVID-19 Following Diphtheria-Tetanus-Pertussis and SARS-CoV-2 Vaccinations in Indonesian Children: Exploring the Roles of Heterologous Immunity.Vaccines (Basel). 2024 Sep 9;12(9):1032. doi: 10.3390/vaccines12091032. Vaccines (Basel). 2024. PMID: 39340062 Free PMC article.
-
SARS-CoV-2 Variants and Their Impact on Pediatric COVID-19: Clinical Manifestations and Hematological Profiles.Diseases. 2025 Feb 6;13(2):48. doi: 10.3390/diseases13020048. Diseases. 2025. PMID: 39997055 Free PMC article.
-
Navigating the shots: Parental willingness to immunize their children with COVID-19 vaccines in Saudi Arabia explored through a systematic review and meta-analysis.PLoS One. 2025 Jan 27;20(1):e0317983. doi: 10.1371/journal.pone.0317983. eCollection 2025. PLoS One. 2025. PMID: 39869589 Free PMC article.
References
-
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. 2021. Available: https://covid19.who.int/. Accessed: 5 February 2024.
-
- World Health Organization. Coronavirus disease (COVID-19): Variants of SARS-COV-2. 2021. Available: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/question.... Accessed: 5 February 2024.
-
- United Nations Children’s Fund. Convention on the Rights of the Child. 1989. Available: https://www.ohchr.org/en/instruments-mechanisms/instruments/convention-r.... Accessed: 5 February 2024.
-
- United Nations Children’s Fund. Investing in a safe, healthy and productive transition from childhood to adulthood is critical. 2022. Available: https://data.unicef.org/topic/adolescents/overview/. Accessed: 5 February 2024.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
