

Effectiveness of Live-Streaming Tele-Exercise Intervention in Patients With Parkinson's Disease: A Pilot Study
- PMID: 38419488
- PMCID: PMC11082614
- DOI: 10.14802/jmd.23251
Effectiveness of Live-Streaming Tele-Exercise Intervention in Patients With Parkinson's Disease: A Pilot Study
Abstract
Objective: Exercise can improve both motor and nonmotor symptoms in people with Parkinson's disease (PwP), but there is an unmet need for accessible and sustainable exercise options. This study aimed to evaluate the effect, feasibility, and safety of a regularly performed live-streaming tele-exercise intervention for PwP.
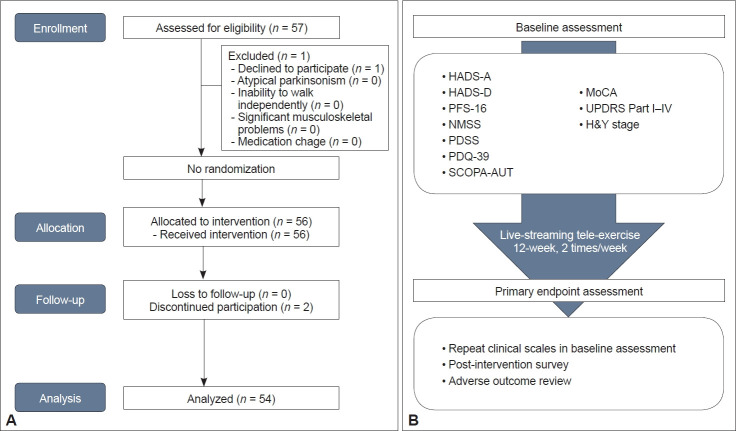
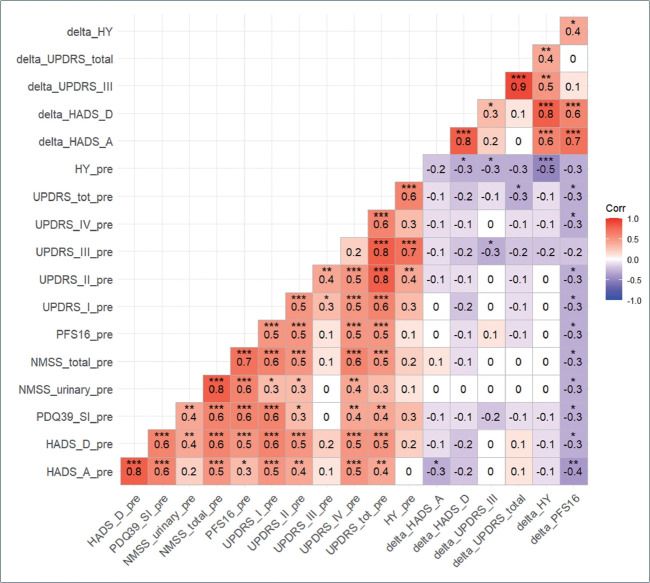
Methods: A live-streaming exercise intervention for PwP was implemented twice a week for 12 weeks. We measured the motor and nonmotor symptom scores of the included patients before and after the intervention. Changes in clinical scores from baseline to postintervention were analyzed using paired t-tests. Factors associated with improvements in clinical scores and compliance were analyzed using Pearson's correlation analysis.
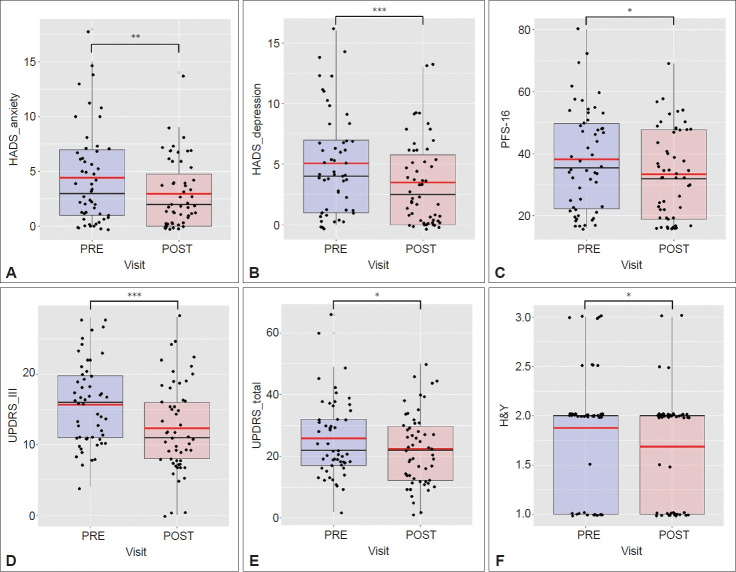
Results: Fifty-six participants were enrolled in the study. There were significant improvements in Hospital Anxiety and Depression Scale (HADS)-anxiety (p = 0.007), HADS-depression (p < 0.001), Unified Parkinson's Disease Rating Scale (UPDRS) part III (p < 0.001), UPDRS total (p = 0.015), Hoehn and Yahr stage (p = 0.027), and Parkinson's Disease Fatigue Scale-16 (p = 0.026) scores after the intervention. Improvements in motor symptoms were associated with improvements in mood symptoms and fatigue. Higher motor impairment at baseline was associated with a greater compliance rate and better postintervention composite motor and nonmotor outcomes (ΔUPDRS total score). Overall, the 12-week tele-exercise program was feasible and safe for PwP. No adverse events were reported. The overall adherence rate was 60.0% in our cohort, and 83.4% of the participants were able to participate in more than half of the exercise routines.
Conclusion: The live-streaming tele-exercise intervention is a safe, feasible, and effective nonpharmacological treatment option that can alleviate fatigue and improve mood and motor symptoms in PwP.
Keywords: Motor symptoms; Nonmotor symptoms; Parkinson’s disease; Tele-exercise; Telehealth.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures
Similar articles
-
Feasibility and acceptability of PDConnect, a multi-component intervention to support physical activity in people with Parkinson's disease: A mixed methods study.J Parkinsons Dis. 2025 May;15(3):603-618. doi: 10.1177/1877718X251324415. Epub 2025 Mar 28. J Parkinsons Dis. 2025. PMID: 40151988 Clinical Trial.
-
Clinical phenotype of drug-naïve Parkinson's disease based on nonmotor symptoms.Arch Gerontol Geriatr. 2015 Nov-Dec;61(3):517-22. doi: 10.1016/j.archger.2015.07.001. Epub 2015 Jul 6. Arch Gerontol Geriatr. 2015. PMID: 26183203
-
A Cross-over Pilot Study on the Effects of Classical Guitar Instruction on Motor and Non-Motor Symptoms in People with Parkinson's Disease.Neurosci Insights. 2025 Mar 24;20:26331055251329878. doi: 10.1177/26331055251329878. eCollection 2025. Neurosci Insights. 2025. PMID: 40143890 Free PMC article.
-
New‑onset non‑motor symptoms in patients with Parkinson's disease and post‑COVID‑19 syndrome: A prospective cross‑sectional study.Med Int (Lond). 2023 Apr 11;3(3):23. doi: 10.3892/mi.2023.83. eCollection 2023 May-Jun. Med Int (Lond). 2023. PMID: 37214229 Free PMC article.
-
Exercise for Older Adults Improves the Quality of Life in Parkinson's Disease and Potentially Enhances the Immune Response to COVID-19.Brain Sci. 2020 Sep 6;10(9):612. doi: 10.3390/brainsci10090612. Brain Sci. 2020. PMID: 32899958 Free PMC article. Review.
Cited by
-
Feasibility and preliminary efficacy of an online home-based functional exercise program for Parkinson's disease: a pilot study.Front Neurol. 2025 Jun 23;16:1591330. doi: 10.3389/fneur.2025.1591330. eCollection 2025. Front Neurol. 2025. PMID: 40625903 Free PMC article.
References
-
- Lee JE, Choi JK, Lim HS, Kim JH, Cho JH, Kim GS, et al. The prevalence and incidence of Parkinson’s disease in South Korea: a 10-year nationwide population–based study. J Korean Neurol Assoc. 2017;35:191–198.
Grants and funding
LinkOut - more resources
Full Text Sources
