

Predicting cervical cancer target motion using a multivariate regression model to enable patient selection for adaptive external beam radiotherapy
- PMID: 38419803
- PMCID: PMC10901141
- DOI: 10.1016/j.phro.2024.100554
Predicting cervical cancer target motion using a multivariate regression model to enable patient selection for adaptive external beam radiotherapy
Abstract
Background and purpose: Interfraction motion during cervical cancer radiotherapy is substantial in some patients, minimal in others. Non-adaptive plans may miss the target and/or unnecessarily irradiate normal tissue. Adaptive radiotherapy leads to superior dose-volume metrics but is resource-intensive. The aim of this study was to predict target motion, enabling patient selection and efficient resource allocation.
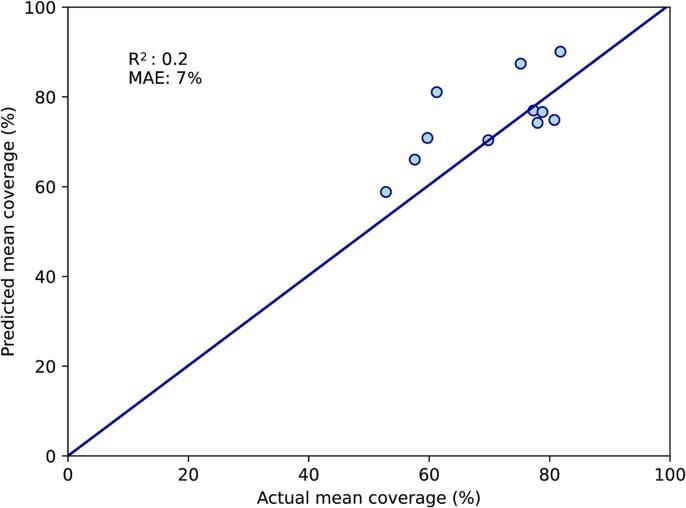
Materials and methods: Forty cervical cancer patients had CT with full-bladder (CT-FB) and empty-bladder (CT-EB) at planning, and daily cone-beam CTs (CBCTs). The low-risk clinical target volume (CTVLR) was contoured. Mean coverage of the daily CTVLR by the CT-FB CTVLR was calculated for each patient. Eighty-three investigated variables included measures of organ geometry, patient, tumour and treatment characteristics. Models were trained on 29 patients (171 fractions). The Two-CT multivariate model could use all available data. The Single-CT multivariate model excluded data from the CT-EB. A univariate model was trained using the distance moved by the uterine fundus tip between CTs, the only method of patient selection found in published cervix plan-of-the-day studies. Models were tested on 11 patients (68 fractions). Accuracy in predicting mean coverage was reported as mean absolute error (MAE), mean squared error (MSE) and R2.
Results: The Two-CT model was based upon rectal volume, dice similarity coefficient between CT-FB and CT-EB CTVLR, and uterine thickness. The Single-CT model was based upon rectal volume, uterine thickness and tumour size. Both performed better than the univariate model in predicting mean coverage (MAE 7 %, 7 % and 8 %; MSE 82 %2, 65 %2, 110 %2; R2 0.2, 0.4, -0.1).
Conclusion: Uterocervix motion is complex and multifactorial. We present two multivariate models which predicted motion with reasonable accuracy using pre-treatment information, and outperformed the only published method.
Keywords: Adaptive radiotherapy; Cervical cancer; Image guided radiotherapy; Interfraction motion; Mathematical modelling.
© 2024 The Author(s).
Conflict of interest statement
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: Lei Wang is part-funded by the National Institute for Health Research (NIHR) Biomedical Research Centre at The Royal Marsden NHS Foundation Trust and The Institute of Cancer Research, London; and part-funded by Elekta Ltd. Helen McNair is funded by a National Institute for Health Research and Health Education England (HEE/NIHR) Senior Clinical Lectureship (ICA-SCL-2018–04-ST2-002). Emma Harris has received research funding from Elekta Ltd and Cancer Research UK Programme Foundation Award A23557. Susan Lalondrelle has received research funding and speaking fees from Elekta Ltd.
Figures







Similar articles
-
Contouring and constraining bowel on a full-bladder computed tomography scan may not reflect treatment bowel position and dose certainty in gynecologic external beam radiation therapy.Int J Radiat Oncol Biol Phys. 2014 Nov 15;90(4):802-8. doi: 10.1016/j.ijrobp.2014.07.016. Epub 2014 Sep 20. Int J Radiat Oncol Biol Phys. 2014. PMID: 25245585
-
Dosimetric advantages of a clinical daily adaptive plan selection strategy compared with a non-adaptive strategy in cervical cancer radiation therapy.Acta Oncol. 2017 May;56(5):667-674. doi: 10.1080/0284186X.2017.1287949. Epub 2017 Feb 20. Acta Oncol. 2017. PMID: 28447562
-
Clinical implementation of an online adaptive plan-of-the-day protocol for nonrigid motion management in locally advanced cervical cancer IMRT.Int J Radiat Oncol Biol Phys. 2014 Nov 1;90(3):673-9. doi: 10.1016/j.ijrobp.2014.06.046. Epub 2014 Aug 20. Int J Radiat Oncol Biol Phys. 2014. PMID: 25151538
-
Image guided adaptive external beam radiation therapy for cervix cancer: Evaluation of a clinically implemented plan-of-the-day technique.Z Med Phys. 2018 Aug;28(3):184-195. doi: 10.1016/j.zemedi.2017.09.004. Epub 2017 Oct 12. Z Med Phys. 2018. PMID: 29031916
-
Clinical Implementation of "Plan of the Day" Strategy in Definitive Radiation Therapy of Cervical Cancer: Online Adaptation to Address the Challenge of Organ Filling Reproducibility.Int J Radiat Oncol Biol Phys. 2024 Mar 1;118(3):605-615. doi: 10.1016/j.ijrobp.2023.09.045. Epub 2023 Oct 9. Int J Radiat Oncol Biol Phys. 2024. PMID: 37816473
Cited by
-
Implementing Plan of the Day for Cervical Cancer: A Comparison of Target Volume Generation Methods.Adv Radiat Oncol. 2024 Jul 1;9(9):101560. doi: 10.1016/j.adro.2024.101560. eCollection 2024 Sep. Adv Radiat Oncol. 2024. PMID: 39155886 Free PMC article.
References
-
- Taylor A., Powell M.E. An assessment of interfractional uterine and cervical motion: implications for radiotherapy target volume definition in gynaecological cancer. Radiother Oncol. 2008;88:250–257. - PubMed
-
- Wang L., Alexander S., Mason S., Blasiak-Wal I., Harris E., McNair H., et al. Carpe diem: making the Most of plan-of-the-day for cervical cancer radiation therapy. Pract Radiat Oncol. 2023;13:132–147. - PubMed
-
- Keall P.J., Nguyen D.T., O'Brien R., Caillet V., Hewson E., Poulsen P.R., et al. The first clinical implementation of real-time image-guided adaptive radiotherapy using a standard linear accelerator. Radiother Oncol. 2018;127:6–11. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
