

A comparison of the performance of 68Ga-Pentixafor PET/CT versus adrenal vein sampling for subtype diagnosis in primary aldosteronism
- PMID: 38419957
- PMCID: PMC10899670
- DOI: 10.3389/fendo.2024.1291775
A comparison of the performance of 68Ga-Pentixafor PET/CT versus adrenal vein sampling for subtype diagnosis in primary aldosteronism
Abstract
Objective: To investigate the diagnostic efficiency and prognostic value of 68Ga-Pentixafor PET/CT in comparison with adrenal vein sampling (AVS) for functional lateralization in primary aldosteronism (PA). Histology and long-term clinical follow-up normally serve as the gold standard for such diagnosis.
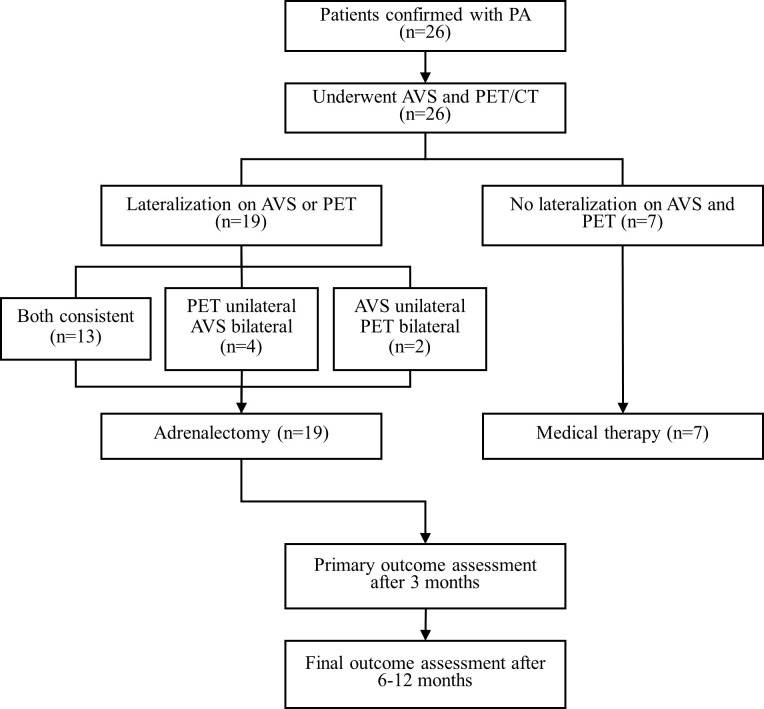
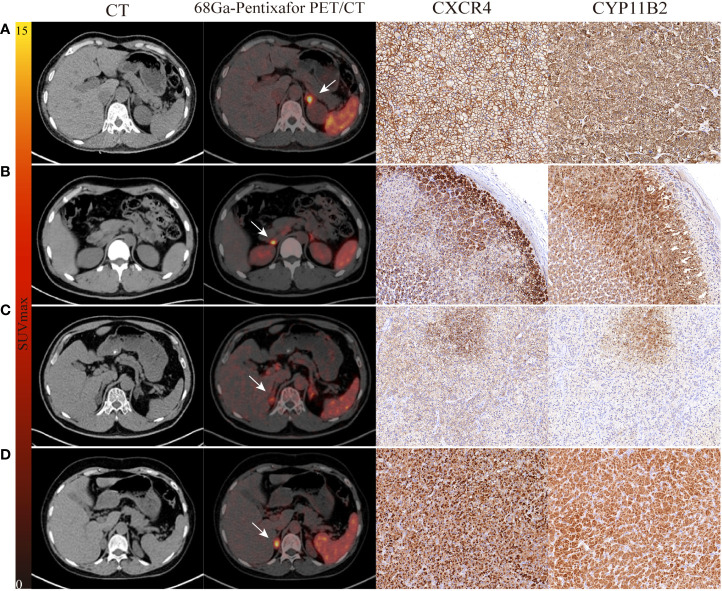
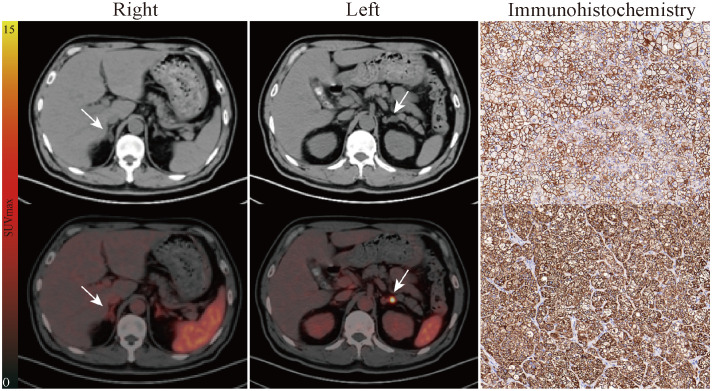
Methods: We prospectively recruited 26 patients diagnosed with PA. All patients underwent 68Ga-Pentixafor PET/CT and AVS. Postsurgical biochemical and clinical outcomes of patients with unilateral primary aldosteronism (UPA), as diagnosed by PET/CT or AVS, were assessed by applying standardized Primary Aldosteronism Surgical Outcome (PASO) criteria. Immunohistochemistry (IHC) was performed to detect the expression of aldosterone synthase (CYP11B2) and CXCR4.
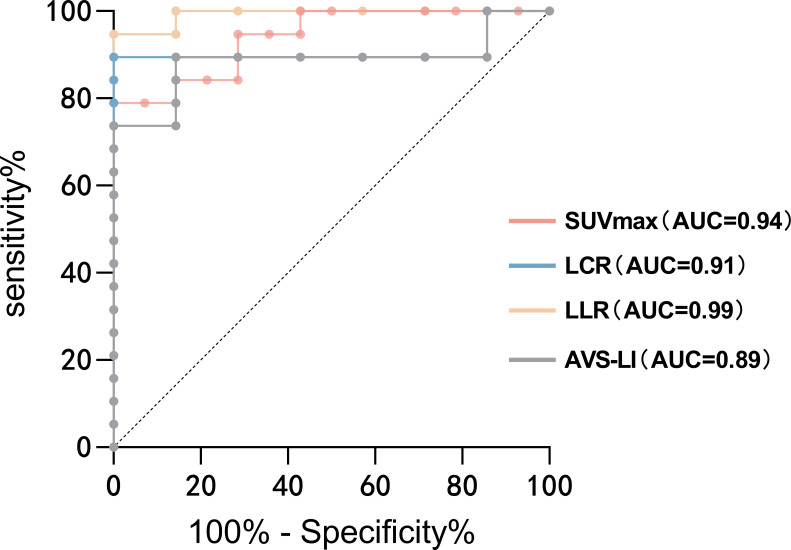
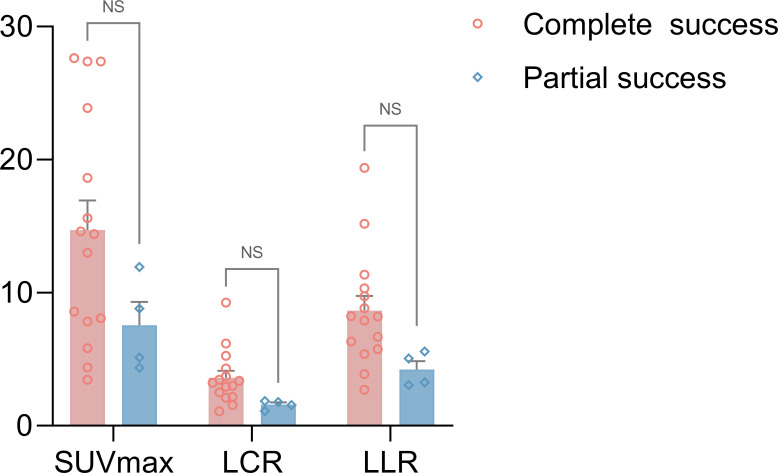
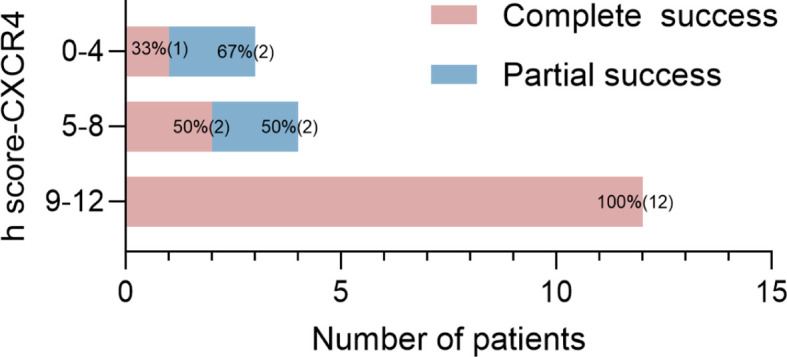
Results: On total, 19 patients were diagnosed with UPA; of these, 13 patients were lateralized by both PET/CT and AVS, four patients were lateralized by PET-only, and two by AVS-only. Seven subjects with no lateralization on AVS and PET received medical therapy. All patients achieved complete biochemical success except one with nodular hyperplasia lateralized by AVS alone. The consistency between PET/CT and AVS outcomes was 77% (20/26). Moreover, CYP11B2-positive nodules were all CXCR4-positive and showed positive findings on PET. Patients who achieved complete biochemical and clinical success had a higher uptake on PET as well as stronger expression levels of CXCR4 and CYP11B2.
Conclusion: Our analysis showed that 68Ga-Pentixafor PET/CT could enable non-invasive diagnosis in most patients with PA and identify additional cases of unilateral and surgically curable PA which could not be classified by AVS. 68Ga-Pentixafor PET/CT should be considered as a first-line test for the future classification of PA.
Keywords: 68Ga-Pentixafor; CXCR4; PET/CT; endocrine hypertension; primary aldosteronism.
Copyright © 2024 Yin, Ai, Luo, Liu, Ma, Zhou, Xiang, Su, Wang and Li.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
CXCR4-directed PET with 68Ga-pentixafor versus adrenal vein sampling for the diagnosis of unilateral primary aldosteronism.Endocrine. 2025 Aug;89(2):603-613. doi: 10.1007/s12020-025-04236-5. Epub 2025 May 19. Endocrine. 2025. PMID: 40388084 Free PMC article.
-
68Ga-pentixafor PET/CT Is a Supplementary Method for Primary Aldosteronism Subtyping Compared with Adrenal Vein Sampling.Mol Imaging Biol. 2025 Feb;27(1):142-150. doi: 10.1007/s11307-024-01976-0. Epub 2024 Dec 23. Mol Imaging Biol. 2025. PMID: 39715984 Free PMC article.
-
Typing diagnostic value of 68Ga-pentixafor PET/CT for patients with primary aldosteronism and unilateral nodules.Endocrine. 2025 Jan;87(1):314-324. doi: 10.1007/s12020-024-04024-7. Epub 2024 Sep 9. Endocrine. 2025. PMID: 39251468
-
Normotensive primary aldosteronism in a patient with myasthenia gravis: a localization diagnostic conundrum unraveled by 68Ga-pentixafor PET/CT - a case report with review of literature.Endocrine. 2025 Jun 10. doi: 10.1007/s12020-025-04311-x. Online ahead of print. Endocrine. 2025. PMID: 40495043 Review.
-
Role of Adrenal Vein Sampling in Guiding Surgical Decision in Primary Aldosteronism.Exp Clin Endocrinol Diabetes. 2023 Aug;131(7-08):418-434. doi: 10.1055/a-2106-4663. Epub 2023 Aug 11. Exp Clin Endocrinol Diabetes. 2023. PMID: 37567230 Review.
Cited by
-
CXCR4-directed PET with 68Ga-pentixafor versus adrenal vein sampling for the diagnosis of unilateral primary aldosteronism.Endocrine. 2025 Aug;89(2):603-613. doi: 10.1007/s12020-025-04236-5. Epub 2025 May 19. Endocrine. 2025. PMID: 40388084 Free PMC article.
-
Case Report: Anomalous drainage vein sampling for diagnosing aldosterone-producing lesions undetectable by segmental adrenal venous sampling in a two-case series.Front Radiol. 2025 Jun 10;5:1567779. doi: 10.3389/fradi.2025.1567779. eCollection 2025. Front Radiol. 2025. PMID: 40557128 Free PMC article.
-
68Ga-pentixafor PET/CT Is a Supplementary Method for Primary Aldosteronism Subtyping Compared with Adrenal Vein Sampling.Mol Imaging Biol. 2025 Feb;27(1):142-150. doi: 10.1007/s11307-024-01976-0. Epub 2024 Dec 23. Mol Imaging Biol. 2025. PMID: 39715984 Free PMC article.
-
The prognostic value of CXCR4 PET/CT imaging in unilateral primary aldosteronism patients after adrenalectomy.EJNMMI Res. 2025 Apr 17;15(1):41. doi: 10.1186/s13550-025-01242-6. EJNMMI Res. 2025. PMID: 40246740 Free PMC article.
-
Clinical diagnosis and treatment of a patient with hypertension, hypokalemia, and bilateral adrenal adenomas.Front Endocrinol (Lausanne). 2025 May 9;16:1558841. doi: 10.3389/fendo.2025.1558841. eCollection 2025. Front Endocrinol (Lausanne). 2025. PMID: 40416524 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous