

Robotic versus open partial pancreatoduodenectomy (EUROPA): a randomised controlled stage 2b trial
- PMID: 38420108
- PMCID: PMC10899052
- DOI: 10.1016/j.lanepe.2024.100864
Robotic versus open partial pancreatoduodenectomy (EUROPA): a randomised controlled stage 2b trial
Abstract
Background: Open partial pancreatoduodenectomy (OPD) represents the current gold standard of surgical treatment of a wide range of diseases of the pancreatic head but is associated with morbidity in around 40% of cases. Robotic partial pancreatoduodenectomy (RPD) is being used increasingly, yet, no randomised controlled trials (RCTs) of RPD versus OPD have been published, leaving a low level of evidence to support this practice.
Methods: This investigator-initiated, exploratory RCT with two parallel study arms was conducted at a high-volume pancreatic centre in line with IDEAL recommendations (stage 2b). Patients scheduled for elective partial pancreatoduodenectomy (PD) for any indication were randomised (1:1) to RPD or OPD with a centralised web-based tool. The primary endpoint was postoperative cumulative morbidity within 90 days, assessed via the Comprehensive Complication Index (CCI). Biometricians were blinded to the intervention, but patients and surgeons were not. The trial was registered prospectively (DRKS00020407).
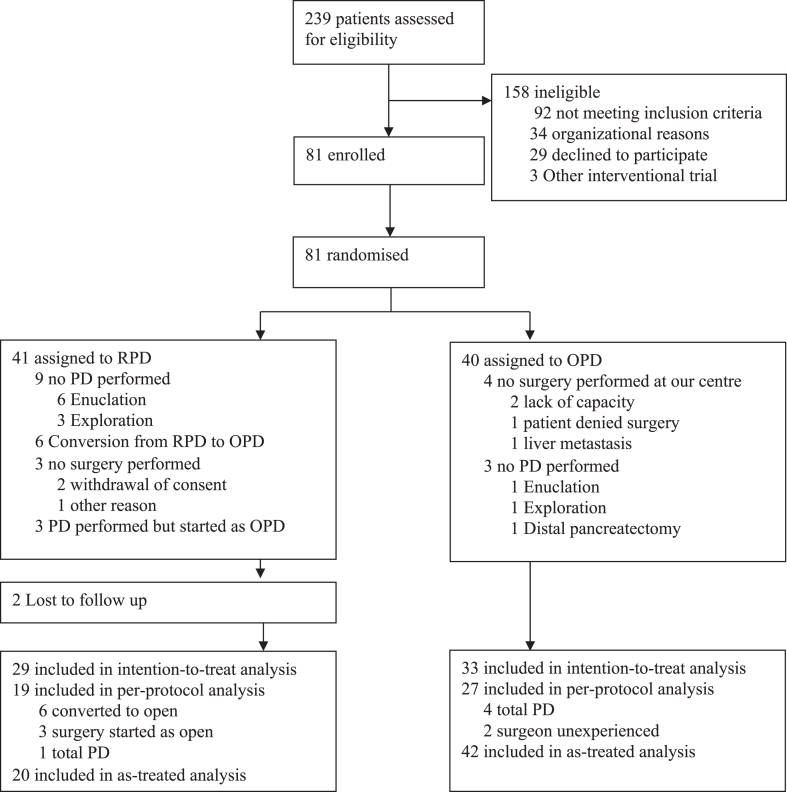
Findings: Between June 3, 2020 and February 14, 2022, 81 patients were randomly assigned to RPD (n = 41) or OPD (n = 40), of whom 62 patients (RPD: n = 29, OPD: n = 33) were analysed in the modified intention to treat analysis. Four patients in the OPD group were randomised, but did not undergo surgery in our department and one patient was excluded in the RPD group due to other reason. Nine patients in the RPD group and 3 patients in the OPD were excluded from the primary analysis because they did not undergo PD, but rather underwent other types of surgery. The CCI after 90 days was comparable between groups (RPD: 34.02 ± 23.48 versus OPD: 36.45 ± 27.65, difference in means [95% CI]: -2.42 [-15.55; 10.71], p = 0.713). The RPD group had a higher incidence of grade B/C pancreas-specific complications compared to the OPD group (17 (58.6%) versus 11 (33.3%); difference in rates [95% CI]: 25.3% [1.2%; 49.4%], p = 0.046). The only complication that occurred significantly more often in the RPD than in the OPD group was clinically relevant delayed gastric emptying. Procedure-related and overall hospital costs were significantly higher and duration of surgery was longer in the RPD group. Blood loss did not differ significantly between groups. The intraoperative conversion rate of RPD was 23%. Overall 90-day mortality was 4.8% without significant differences between RPD and OPD.
Interpretation: In the setting of a very high-volume centre, both RPD and OPD can be considered safe techniques. Further confirmatory multicentre RCTs are warranted to uncover potential advantages of RPD in terms of perioperative and long-term outcomes.
Funding: Federal Ministry of Education and Research (BMBF: 01KG2010).
Keywords: Open; Pancreas; Partial pancreatoduodenectomy; Randomised controlled trial; Robotic.
© 2024 The Author(s).
Conflict of interest statement
All authors have completed the ICMJE uniform disclosure form at http://www.icmje.org/disclosure-of-interest/and declare: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures
Comment in
-
Feasibility and outcomes of robotic partial pancreatoduodenectomy.Hepatobiliary Surg Nutr. 2024 Aug 1;13(4):669-671. doi: 10.21037/hbsn-24-288. Epub 2024 Jul 16. Hepatobiliary Surg Nutr. 2024. PMID: 39175737 Free PMC article. No abstract available.
References
-
- Mariette C., Markar S.R., Dabakuyo-Yonli T.S., et al. Hybrid minimally invasive esophagectomy for esophageal cancer. N Engl J Med. 2019;380(2):152–162. - PubMed
-
- Asbun H.J., Moekotte A.L., Vissers F.L., et al. The Miami international evidence-based guidelines on minimally invasive pancreas resection. Ann Surg. 2020;271(1):1–14. - PubMed
-
- de Rooij T., van Hilst J., van Santvoort H., et al. Minimally invasive versus open distal pancreatectomy (leopard): a multicenter patient-blinded randomized controlled trial. Ann Surg. 2019;269(1):2–9. - PubMed
-
- Bjornsson B., Larsson A.L., Hjalmarsson C., Gasslander T., Sandstrom P. Comparison of the duration of hospital stay after laparoscopic or open distal pancreatectomy: randomized controlled trial. Br J Surg. 2020;107(10):1281–1288. - PubMed
LinkOut - more resources
Full Text Sources
Medical
