

Why so Many Patients With Dysphagia Have Normal Esophageal Function Testing
- PMID: 38420259
- PMCID: PMC10899865
- DOI: 10.1016/j.gastha.2023.08.021
Why so Many Patients With Dysphagia Have Normal Esophageal Function Testing
Abstract
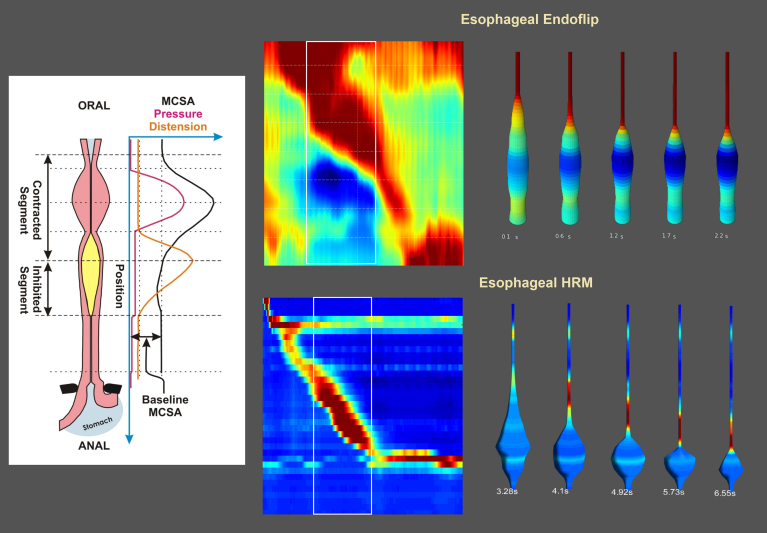
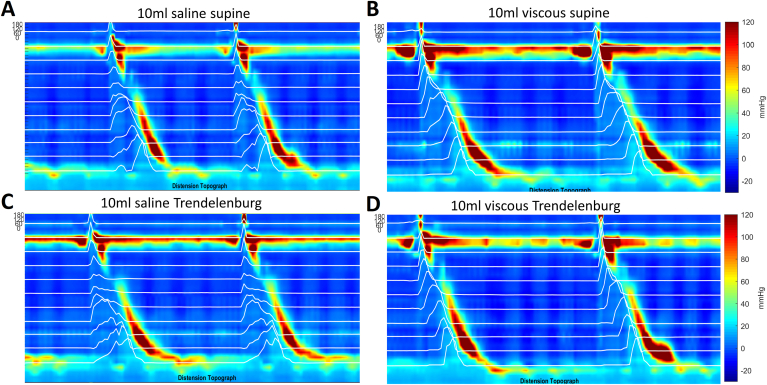
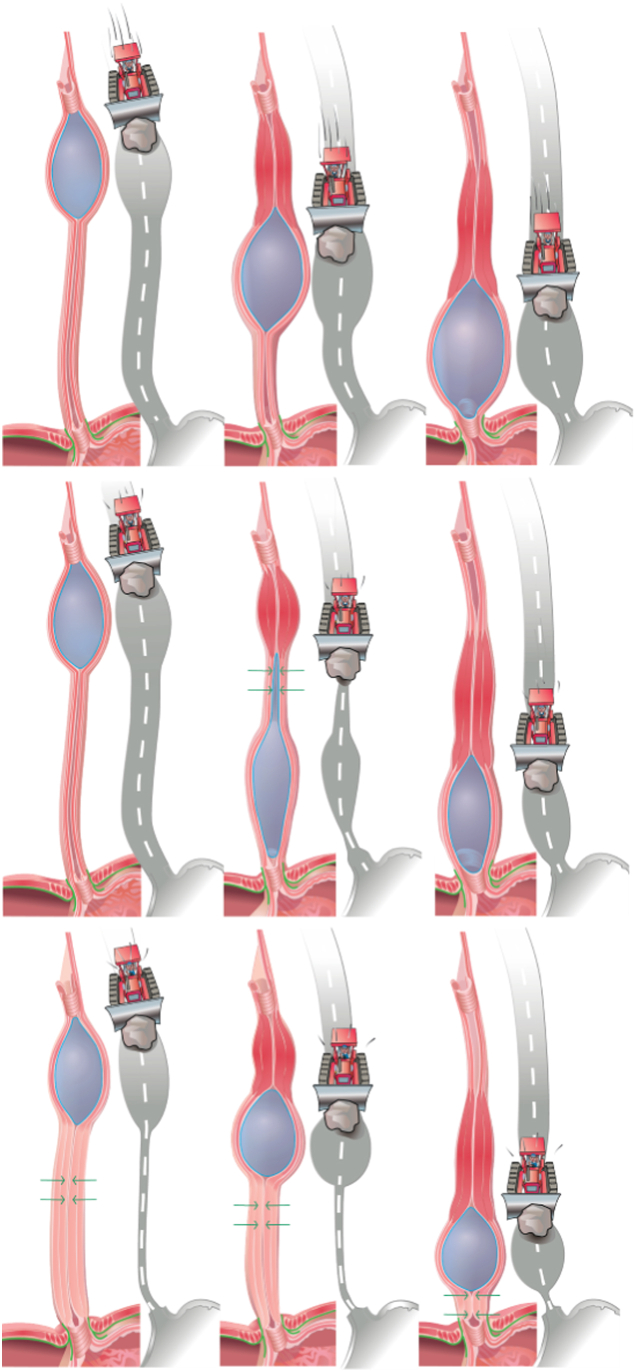
Esophageal peristalsis involves a sequential process of initial inhibition (relaxation) and excitation (contraction), both occurring from the cranial to caudal direction. The bolus induces luminal distension during initial inhibition (receptive relaxation) that facilitates smooth propulsion by contraction travelling behind the bolus. Luminal distension during peristalsis in normal subjects exhibits unique characteristics that are influenced by bolus volume, bolus viscosity, and posture, suggesting a potential interaction between distension and contraction. Examining distension-contraction plots in dysphagia patients with normal bolus clearance, ie, high-amplitude esophageal peristaltic contractions, esophagogastric junction outflow obstruction, and functional dysphagia, reveal 2 important findings. Firstly, patients with type 3 achalasia and nonobstructive dysphagia show luminal occlusion distal to the bolus during peristalsis. Secondly, patients with high-amplitude esophageal peristaltic contractions, esophagogastric junction outflow obstruction, and functional dysphagia exhibit a narrow esophageal lumen through which the bolus travels during peristalsis. These findings indicate a relative dynamic obstruction to bolus flow and reduced distensibility of the esophageal wall in patients with several primary esophageal motility disorders. We speculate that the dysphagia sensation experienced by many patients may result from a normal or supernormal contraction wave pushing the bolus against resistance. Integrating representations of distension and contraction, along with objective assessments of flow timing and distensibility, complements the current classification of esophageal motility disorders that are based on the contraction characteristics only. A deeper understanding of the distensibility of the bolus-containing esophageal segment during peristalsis holds promise for the development of innovative medical and surgical therapies to effectively address dysphagia in a substantial number of patients.
Keywords: Distension Contration Plot; Dysphagia; Esophageal Peristalsis; Functional Dysphagia.
Conflict of interest statement
Conflicts of Interest: Ravinder K. Mittal and Ali Zifan have copyright/patent protection for the computer software (Dplots). Ravinder K. Mittal is a member of the Board of Editors. Their paper was handled in accordance with our conflict of interest policy. See https://www.ghadvances.org/content/authorinfo#conflict_of_interest_policy for full details.
Figures




Comment in
-
Functional Dysphagia Loses the Functional.Gastro Hep Adv. 2023 Dec 4;3(1):136-137. doi: 10.1016/j.gastha.2023.12.001. eCollection 2024. Gastro Hep Adv. 2023. PMID: 39132180 Free PMC article. No abstract available.
Similar articles
-
Distension contraction plots of pharyngeal/esophageal peristalsis: next frontier in the assessment of esophageal motor function.Am J Physiol Gastrointest Liver Physiol. 2022 Sep 1;323(3):G145-G156. doi: 10.1152/ajpgi.00124.2022. Epub 2022 Jul 5. Am J Physiol Gastrointest Liver Physiol. 2022. PMID: 35788152 Free PMC article. Review.
-
Esophageal wall compliance/stiffness during peristalsis in patients with functional dysphagia and high-amplitude esophageal contractions.Am J Physiol Gastrointest Liver Physiol. 2022 Dec 1;323(6):G586-G593. doi: 10.1152/ajpgi.00075.2022. Epub 2022 Oct 25. Am J Physiol Gastrointest Liver Physiol. 2022. PMID: 36283085 Free PMC article.
-
Rhythmic contraction but arrhythmic distension of esophageal peristaltic reflex in patients with dysphagia.PLoS One. 2022 Jan 24;17(1):e0262948. doi: 10.1371/journal.pone.0262948. eCollection 2022. PLoS One. 2022. PMID: 35073388 Free PMC article. Clinical Trial.
-
Relationship between distension-contraction waveforms during esophageal peristalsis: effect of bolus volume, viscosity, and posture.Am J Physiol Gastrointest Liver Physiol. 2020 Oct 1;319(4):G454-G461. doi: 10.1152/ajpgi.00117.2020. Epub 2020 Aug 5. Am J Physiol Gastrointest Liver Physiol. 2020. PMID: 32755311 Free PMC article.
-
[Pharmacological Treatments of Esophageal Dysphagia].Korean J Gastroenterol. 2021 Feb 25;77(2):71-76. doi: 10.4166/kjg.2021.024. Korean J Gastroenterol. 2021. PMID: 33632997 Review. Korean.
Cited by
-
When Manometry and Functional Lumen Imaging Probe Disagree: The Current Limitations of the Chicago Classification Version 4.0 and Probable Extended Indications of Functional Lumen Imaging Probe.J Neurogastroenterol Motil. 2025 Jul 30;31(3):304-312. doi: 10.5056/jnm25054. Epub 2025 Apr 18. J Neurogastroenterol Motil. 2025. PMID: 40254534 Free PMC article. Review.
-
Functional Dysphagia Loses the Functional.Gastro Hep Adv. 2023 Dec 4;3(1):136-137. doi: 10.1016/j.gastha.2023.12.001. eCollection 2024. Gastro Hep Adv. 2023. PMID: 39132180 Free PMC article. No abstract available.
-
Esophageal and Oropharyngeal Dysphagia: Clinical Recommendations From the United European Gastroenterology and European Society for Neurogastroenterology and Motility.United European Gastroenterol J. 2025 Jul;13(6):855-901. doi: 10.1002/ueg2.70062. Epub 2025 Jun 21. United European Gastroenterol J. 2025. PMID: 40543044 Free PMC article.
References
-
- Camilleri M., Dubois D., Coulie B., et al. Prevalence and socioeconomic impact of upper gastrointestinal disorders in the United States: results of the US Upper Gastrointestinal Study. Clin Gastroenterol Hepatol. 2005;3:543–552. - PubMed
-
- Eslick G.D., Talley N.J. Dysphagia: epidemiology, risk factors and impact on quality of life--a population-based study. Aliment Pharmacol Ther. 2008;27:971–979. - PubMed
-
- Chiocca J.C., Olmos J.A., Salis G.B., et al. Prevalence, clinical spectrum and atypical symptoms of gastro-oesophageal reflux in Argentina: a nationwide population-based study. Aliment Pharmacol Ther. 2005;22:331–342. - PubMed
-
- Wong W.M., Lai K.C., Lam K.F., et al. Prevalence, clinical spectrum and health care utilization of gastro-oesophageal reflux disease in a Chinese population: a population-based study. Aliment Pharmacol Ther. 2003;18:595–604. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
