

Adherence to clinical practice guidelines for pulmonary valve intervention after tetralogy of Fallot repair: A nationwide cohort study
- PMID: 38420530
- PMCID: PMC10897679
- DOI: 10.1016/j.xjon.2023.11.013
Adherence to clinical practice guidelines for pulmonary valve intervention after tetralogy of Fallot repair: A nationwide cohort study
Abstract
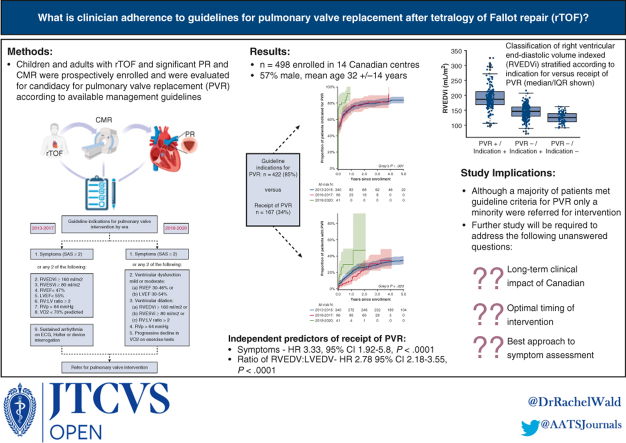
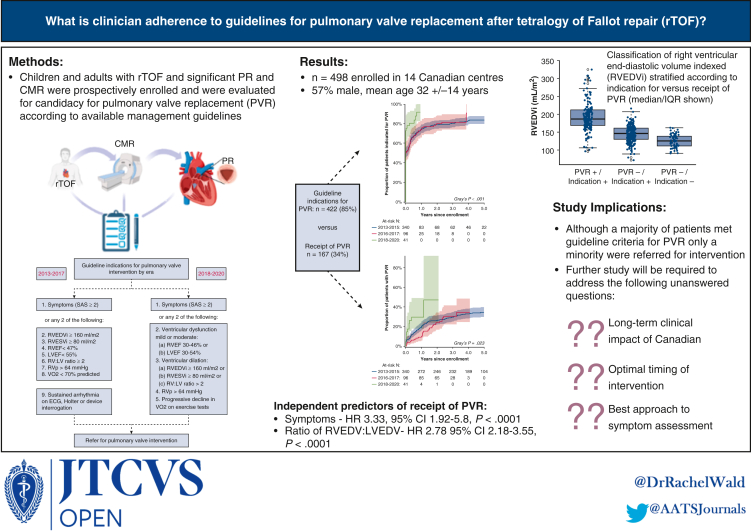
Objectives: To determine guideline adherence pertaining to pulmonary valve replacement (PVR) referral after tetralogy of Fallot (TOF) repair.
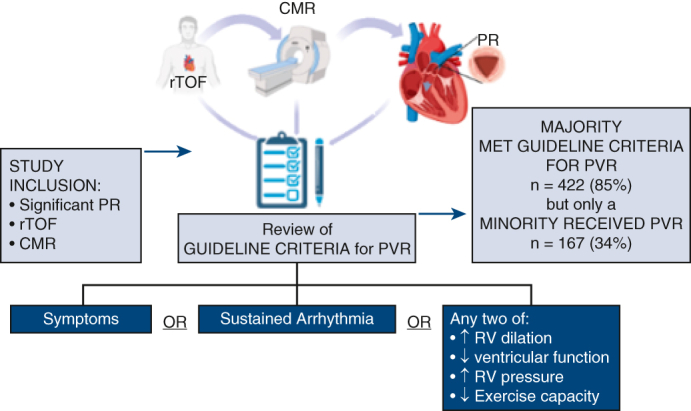
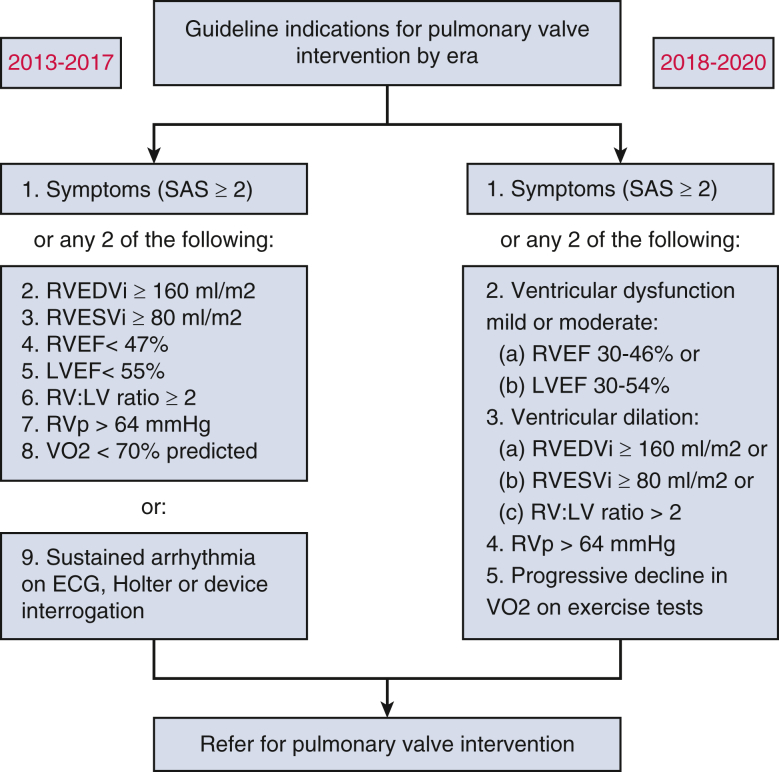
Methods: Children and adults with cardiovascular magnetic resonance imaging scans and at least moderate pulmonary regurgitation were prospectively enrolled in the Comprehensive Outcomes Registry Late After TOF Repair (CORRELATE). Individuals with previous PVR were excluded. Patients were classified according to presence (+) versus absence (-) of PVR and presence (+) versus absence (-) of contemporaneous guideline satisfaction. A validated score (specific activity scale [SAS]) classified adult symptom status.
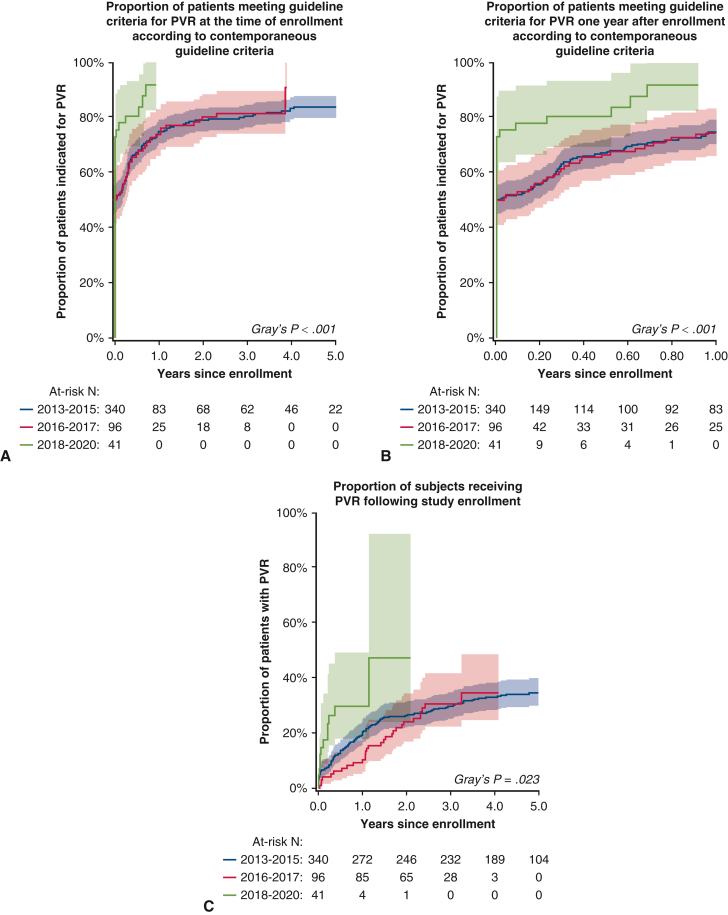
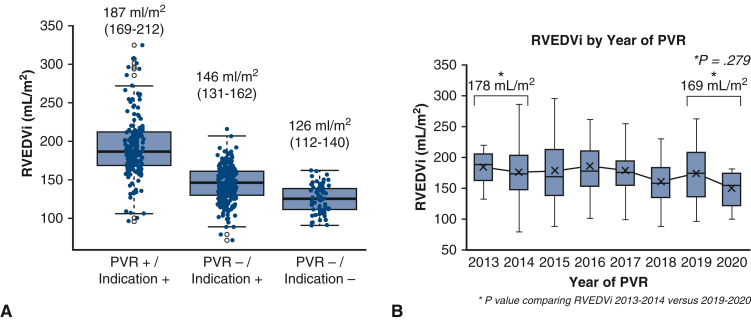
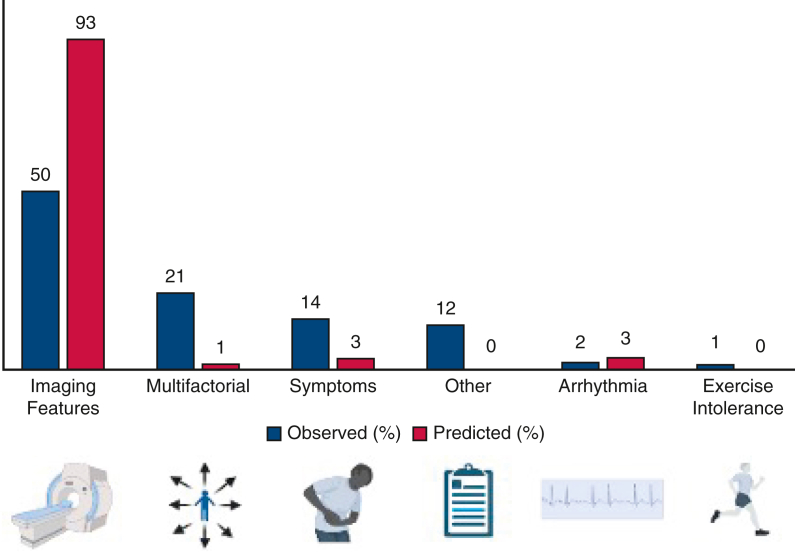
Results: In total, 498 participants (57% male, mean age 32 ± 14 years) were enrolled from 14 Canadian centers (2013-2020). Mean follow-up was 3.8 ± 1.8 years. Guideline criteria for PVR were satisfied for the majority (n = 422/498, 85%), although referral for PVR occurred only in a minority (n = 167/498, 34%). At PVR referral, most were asymptomatic (75% in SAS class 1). One participant (0.6%) received PVR without meeting criteria (PVR+/indication-). The remainder (n = 75/498, 15%) did not meet criteria for and did not receive PVR (PVR-/indication-). Abnormal cardiovascular imaging was the most commonly cited indication for PVR (n = 61/123, 50%). The SAS class and ratio of right to left end-diastolic volumes were independent predictors of PVR in a multivariable analysis (hazard ratio, 3.33; 95% confidence interval, 1.92-5.8, P < .0001; hazard ratio, 2.78; 95% confidence interval, 2.18-3.55, P < .0001).
Conclusions: Although a majority of patients met guideline criteria for PVR, only a minority were referred for intervention. Abnormal cardiovascular imaging was the most common indication for referral. Further research will be necessary to establish the longer-term clinical impact of varying PVR referral strategies.
Keywords: cardiac MRI; guidelines; pulmonary valve replacement; tetralogy of Fallot.
© 2023 The Author(s).
Conflict of interest statement
The authors reported no conflicts of interest. The Journal policy requires editors and reviewers to disclose conflicts of interest and to decline handling or reviewing manuscripts for which they may have a conflict of interest. The editors and reviewers of this article have no conflicts of interest.
Figures
References
-
- Warnes C.A., Williams R.G., Bashore T.M., Child J.S., Connolly H.M., Dearani J.A., et al. ACC/AHA 2008 guidelines for the management of adults with congenital heart disease: a report of the American College of Cardiology/American Heart Association task force on practice guidelines (writing committee to develop guidelines on the management of adults with congenital heart disease). Developed in collaboration with the American Society of Echocardiography, Heart Rhythm Society, International Society for Adult Congenital Heart Disease, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol. 2008;52:e143–e263. - PubMed
-
- Stout K.K., Daniels C.J., Aboulhosn J.A., Bozkurt B., Broberg C.S., Colman J.M., et al. 2018 AHA/ACC guideline for the management of adults with congenital heart disease: executive summary: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines. J Am Coll Cardiol. 2019;73:1494–1563. - PubMed
-
- Wald R.M., Altaha M.A., Alvarez N., Caldarone C.A., Cavallé-Garrido T., Dallaire F., et al. Rationale and design of the Canadian Outcomes Registry late after tetralogy of Fallot repair: the CORRELATE study. Can J Cardiol. 2014;30:1436–1443. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
