

Outcomes of minimally invasive isolated tricuspid valve repair and replacement through right mini-thoracotomy
- PMID: 38420554
- PMCID: PMC10897664
- DOI: 10.1016/j.xjon.2023.12.009
Outcomes of minimally invasive isolated tricuspid valve repair and replacement through right mini-thoracotomy
Abstract
Objective: Isolated tricuspid valve surgery is uncommon and associated with high perioperative morbidity and mortality. We aimed to study the overall outcomes of patients who underwent minimally invasive right thoracotomy tricuspid valve surgery (Mini-TVS), consisting of either tricuspid valve repair (TVre) or replacement (TVR).
Methods: We performed a retrospective analysis of all Mini-TVS procedures (2017-2022), through which we identified isolated tricuspid valve surgeries. We examined in-hospital outcomes, survival analysis over a 4-year period, and competing risk analysis for reoperative surgery.
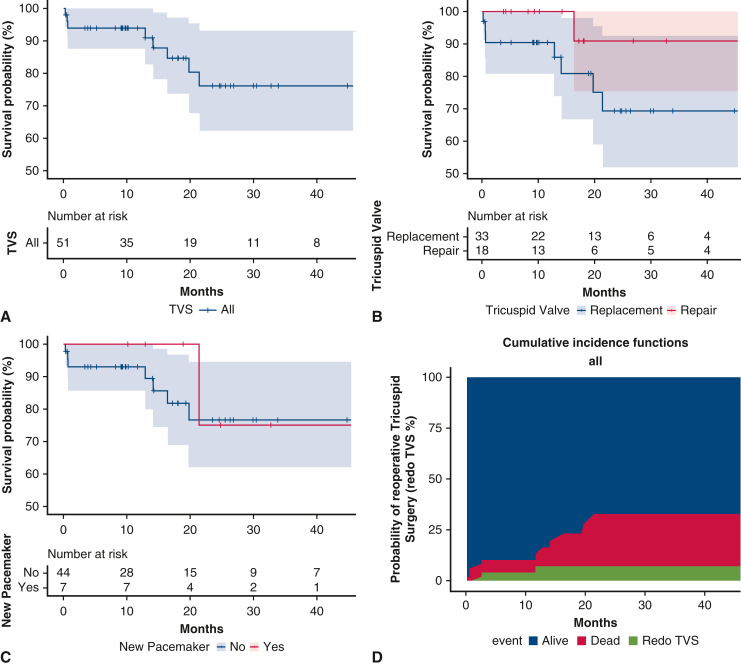
Results: Among a total of 51 patients, the average age was 60 ± 16 years, and 67% (n = 34) were female. Severe tricuspid regurgitation was present in all cases. Infective endocarditis was noted in 7.8% (n = 4), and 24% (n = 12) had preexisting pacemakers. Mini-TVS included TVre in 18 patients (35%) and TVR in 33 patients (65%). The in-hospital and 30-day mortality rates were 4% (n = 2) and 6% (n = 3), respectively. At 4 years, the overall TVS survival was 76% (confidence interval, 62-93%), with no significant difference between TVre and TVR (91% vs 69%, P = .16). At follow-up, 3 patients required repeat surgery for recurrent regurgitation after 2.6, 3.3, and 11 months, with a reoperation rate of 7.3% (confidence interval, 2.4-22%) at 2 years. Factors associated with worse overall survival included nonelective surgery, right ventricular dysfunction, serum creatinine >2 g/dL, and concomitant left-sided valve disease.
Conclusions: A nonsternotomy minimally invasive approach is a feasible option for high-risk patients. Midterm outcomes were similar in repair or replacement. Patients with right ventricular dysfunction and left-sided disease had worse outcomes.
Keywords: isolated tricuspid; minimally invasive; outcomes; survival; tricuspid valve.
© 2023 The Author(s).
Conflict of interest statement
Dr Lamelas reported receiving honoraria as a speaker for Edwards and Medtronic as well as owning stocks and on the medical advisory board of Cardiac Success. All other authors reported no conflicts of interest. The Journal policy requires editors and reviewers to disclose conflicts of interest and to decline handling or reviewing manuscripts for which they may have a conflict of interest. The editors and reviewers of this article have no conflicts of interest.
Figures


References
-
- LaPietra A., Santana O., Mihos C.G., DeBeer S., Rosen G.P., Lamas G.A., et al. Incidence of cerebrovascular accidents in patients undergoing minimally invasive valve surgery. J Thorac Cardiovasc Surg. 2014;148:156–160. - PubMed
-
- Lamelas J., Alnajar A. Recent advances in devices for minimally invasive aortic valve replacement. Expert Rev Med Devices. 2020;17:201–208. - PubMed
-
- Lamelas J., Sarria A., Santana O., Pineda A.M., Lamas G.A. Outcomes of minimally invasive valve surgery versus median sternotomy in patients age 75 years or greater. Ann Thorac Surg. 2011;91:79–84. - PubMed
-
- Cheng D.C., Martin J., Lal A., Diegeler A., Folliguet T.A., Nifong L.W., et al. Minimally invasive versus conventional open mitral valve surgery: a meta-analysis and systematic review. Innovations (Phila) 2011;6:84–103. - PubMed
E-References
-
- Therneau T. A package for survival analysis in R. R package version 3.5-3. 2023. https://CRAN.R-project.org/package=survival
-
- Gray B. cmprsk: subdistribution analysis of competing risks. R package version 2.2-11. 2022. https://CRAN.R-project.org/package=cmprsk
-
- Kassambara A., Kosinski M., Biecek P. survminer: drawing survival curves using ‘ggplot2’. R package version 0.4.9. 2021. https://CRAN.R-project.org/package=survminer
-
- Sjoberg D.D., Whiting K., Curry M., Lavery J.A., Larmarange J. Reproducible summary tables with the gtsummary package. R J. 2021;13:570–580. doi: 10.32614/RJ-2021-053. - DOI
-
- Gohel D. flextable: functions for tabular reporting. R package version 0.7.2. 2022. https://CRAN.R-project.org/package=flextable
LinkOut - more resources
Full Text Sources
