

Multivariate prognostic index and triplet regimen efficacy predictive index in locally advanced and metastatic gastric cancer: pooled analysis from three clinical trials using individual patient data
- PMID: 38420603
- PMCID: PMC10901054
- DOI: 10.1177/17588359241233982
Multivariate prognostic index and triplet regimen efficacy predictive index in locally advanced and metastatic gastric cancer: pooled analysis from three clinical trials using individual patient data
Abstract
Background: To construct an effective prognostic index to predict overall survival (OS) and triplet regimen efficacy for advanced gastric cancer (AGC) patients treated with platinum-based and fluorouracil-based chemotherapy.
Objectives: Between 2011 and 2021, 679 patients from two randomized phase III trials and one phase II trial were enrolled.
Designs: We collected 11 baseline clinicopathological and 14 hematological parameters to establish a prognostic index.
Methods: Univariate and multivariate Cox analyses were used to screen prognostic factors, and a prognostic index nomogram was conducted.
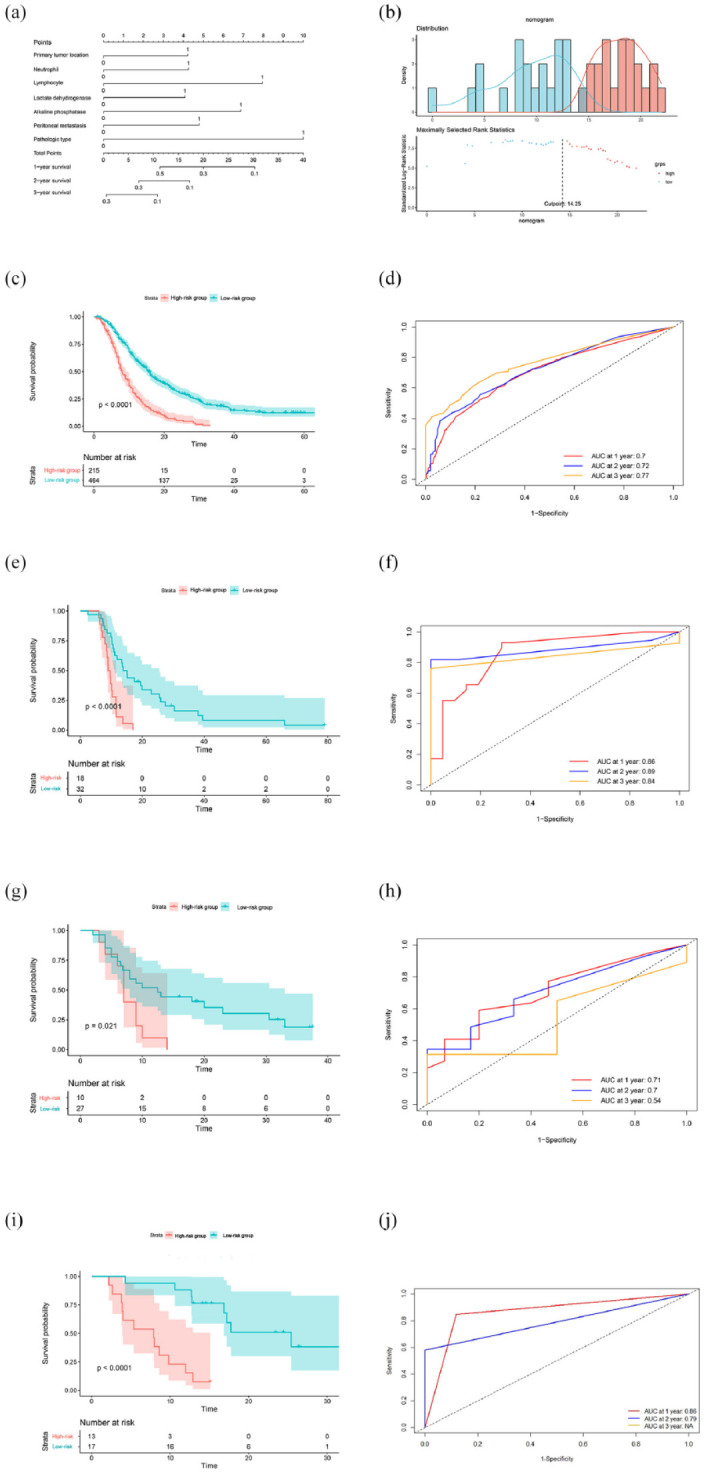
Results: Seven prognostic factors were identified: primary tumor site in the non-proximal gastric area, signet-ring cell carcinoma (SRCC)/mucinous carcinoma, peritoneal metastasis, neutrophil count higher than the upper limit of normal value (ULN), lymphocyte count lower than the lower limit of normal value, lactate dehydrogenase level higher than the ULN, and alkaline phosphatase level higher than the ULN as significant for prognosis. A prognostic nomogram named the Fudan advanced gastric cancer prognostic risk score (FARS) index was constructed, and patients in the high-risk group had significantly shorter OS than those in the low-risk group (median OS, 15.5 versus 8.0 months, p < 0.001). The areas under the curve of the FARS index for 1-, 2-, and 3-year OS were 0.70, 0.72, and 0.77, respectively. A validation and external cohort verified the prognostic value of the FARS index. Moreover, three triplet regimen efficacy parameters were identified: SRCC/mucinous adenocarcinoma, primary tumor location in the non-proximal gastric area, and peripheral neutrophil count higher than the ULN; a TRIS index was subsequently conducted. In patients with any two of the three parameters, the triplet regimen showed significantly longer OS than the doublet regimen (p = 0.018).
Conclusion: The constructed FARS index to predict the OS of AGC patients and the TRIS index to screen out the dominant population for triplet regimens can be used to aid clinical decision-making and individual risk stratification.
Keywords: advanced gastric cancer; chemotherapy; overall survival; prognostic index; triplet regimen efficacy predictive index.
Plain language summary
A prognostic index in locally advanced and metastatic gastric cancer To date, no recognized systematic prognostic score has been established for advanced gastric cancer (AGC). Our research aims to construct an effective prognostic index to predict overall survival (OS) for AGC patients to aid clinical decision-making and individual risk stratification. In our research, seven prognostic factors were identified: primary tumor site in the non-proximal gastric area, signet-ring cell carcinoma (SRCC)/mucinous carcinoma, peritoneal metastasis, neutrophil count higher than the upper limit of normal value (ULN), lymphocyte count lower than the lower limit of normal value, lactate dehydrogenase level higher than the ULN, and alkaline phosphatase level higher than the ULN as significant for prognosis. A prognostic index named the Fudan advanced gastric cancer prognostic risk score (FARS) index was constructed, and patients in the high-risk group had significantly shorter OS than those in low-risk group (median OS, 15.5 months vs. 8.0 months, P < 0.001). Moreover, three triplet regimen efficacy parameters were identified: SRCC/mucinous adenocarcinoma, primary tumor location in the non-proximal gastric area, and peripheral neutrophil count higher than the ULN; a TRIS index was subsequently conducted. In patients with any two of the three parameters, the triplet regimen showed significantly longer OS than the doublet regimen (P = 0.018).
© The Author(s), 2024.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Figures



Similar articles
-
The percentages of signet-ring cells (SRCs) affects the prognosis after radical gastrectomy for advanced gastric cancer.Langenbecks Arch Surg. 2023 Sep 25;408(1):376. doi: 10.1007/s00423-023-03114-w. Langenbecks Arch Surg. 2023. PMID: 37743407
-
Comparison of clinicopathological and prognostic characteristics in patients with mucinous carcinoma and signet ring cell carcinoma of the stomach.Curr Med Res Opin. 2017 Jan;33(1):109-116. doi: 10.1080/03007995.2016.1239192. Epub 2016 Oct 18. Curr Med Res Opin. 2017. PMID: 27646639
-
A Retrospective Study of Neoadjuvant Chemotherapy for Locally Advanced Gastric Cancer.Cancer Manag Res. 2020 Sep 15;12:8491-8496. doi: 10.2147/CMAR.S267330. eCollection 2020. Cancer Manag Res. 2020. PMID: 32982442 Free PMC article.
-
Capecitabine for the treatment of advanced gastric cancer.Health Technol Assess. 2010 Oct;14(Suppl. 2):11-7. doi: 10.3310/hta14suppl2/02. Health Technol Assess. 2010. PMID: 21047486 Review.
-
Microangiopathic Hemolytic Anemia Is a Late and Fatal Complication of Gastric Signet Ring Cell Carcinoma: A Systematic Review and Case-Control Study.Oncologist. 2022 Sep 2;27(9):751-759. doi: 10.1093/oncolo/oyac093. Oncologist. 2022. PMID: 35589098 Free PMC article.
References
-
- Wöhrer SS, Raderer M, Hejna M .Palliative chemotherapy for advanced gastric cancer. Ann Oncol 2004; 15: 1585–1595. - PubMed
-
- Rizzo A, Mollica V, Ricci AD, et al.. Third- and later-line treatment in advanced or metastatic gastric cancer: a systematic review and meta-analysis. Future Oncol 2020; 16: 4409–4418. - PubMed
-
- Chau I, Norman AR, Cunningham D, et al.. Multivariate prognostic factor analysis in locally advanced and metastatic esophago-gastric cancer—pooled analysis from three multicenter, randomized, controlled trials using individual patient data. J Clin Oncol 2004; 22: 2395–2403. - PubMed
-
- Webb A, Cunningham D, Scarffe JH, et al.. Randomized trial comparing epirubicin, cisplatin, and fluorouracil versus fluorouracil, doxorubicin, and methotrexate in advanced esophagogastric cancer. J Clin Oncol 1997; 15: 261–267. - PubMed
LinkOut - more resources
Full Text Sources
