

Proteomic Associations of Adverse Outcomes in Human Heart Failure
- PMID: 38420755
- PMCID: PMC10944037
- DOI: 10.1161/JAHA.123.031154
Proteomic Associations of Adverse Outcomes in Human Heart Failure
Abstract
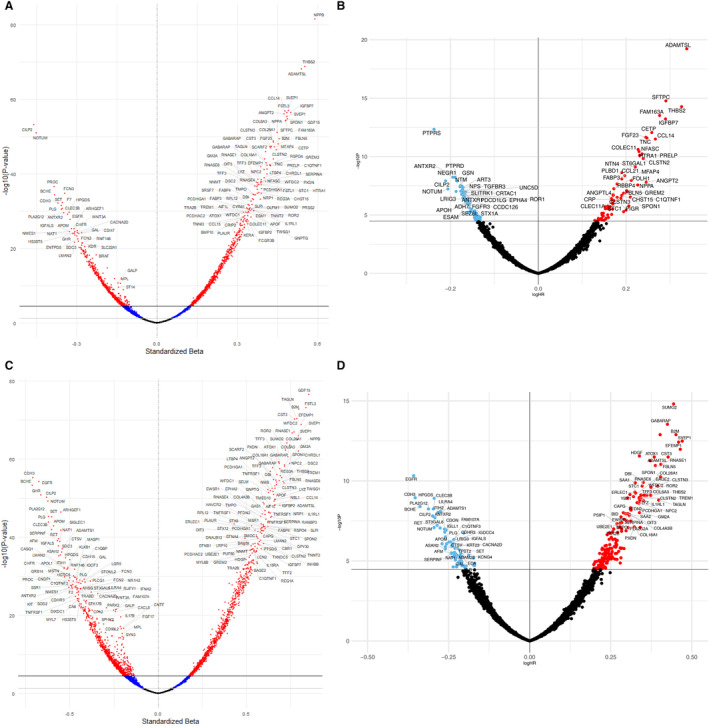
Background: Identifying novel molecular drivers of disease progression in heart failure (HF) is a high-priority goal that may provide new therapeutic targets to improve patient outcomes. The authors investigated the relationship between plasma proteins and adverse outcomes in HF and their putative causal role using Mendelian randomization.
Methods and results: The authors measured 4776 plasma proteins among 1964 participants with HF with a reduced left ventricular ejection fraction enrolled in PHFS (Penn Heart Failure Study). Assessed were the observational relationship between plasma proteins and (1) all-cause death or (2) death or HF-related hospital admission (DHFA). The authors replicated nominally significant associations in the Washington University HF registry (N=1080). Proteins significantly associated with outcomes were the subject of 2-sample Mendelian randomization and colocalization analyses. After correction for multiple testing, 243 and 126 proteins were found to be significantly associated with death and DHFA, respectively. These included small ubiquitin-like modifier 2 (standardized hazard ratio [sHR], 1.56; P<0.0001), growth differentiation factor-15 (sHR, 1.68; P<0.0001) for death, A disintegrin and metalloproteinase with thrombospondin motifs-like protein (sHR, 1.40; P<0.0001), and pulmonary-associated surfactant protein C (sHR, 1.24; P<0.0001) for DHFA. In pathway analyses, top canonical pathways associated with death and DHFA included fibrotic, inflammatory, and coagulation pathways. Genomic analyses provided evidence of nominally significant associations between levels of 6 genetically predicted proteins with DHFA and 11 genetically predicted proteins with death.
Conclusions: This study implicates multiple novel proteins in HF and provides preliminary evidence of associations between genetically predicted plasma levels of 17 candidate proteins and the risk for adverse outcomes in human HF.
Keywords: HFrEF; Mendelian randomization; heart failure; proteomics.
Figures







References
-
- Tsao CW, Aday AW, Almarzooq ZI, Alonso A, Beaton AZ, Bittencourt MS, Boehme AK, Buxton AE, Carson AP, Commodore‐Mensah Y, et al. Heart disease and stroke statistics‐2022 update: a report from the American Heart Association. Circulation. 2022;145:e153–e639. doi: 10.1161/CIR.0000000000001052 - DOI - PubMed
-
- Bozkurt B, Coats AJ, Tsutsui H, Abdelhamid M, Adamopoulos S, Albert N, Anker SD, Atherton J, Bohm M, Butler J, et al. Universal definition and classification of heart failure: a report of the Heart Failure Society of America, Heart Failure Association of the European Society of Cardiology, Japanese Heart Failure Society and Writing Committee of the Universal Definition of Heart Failure. J Card Fail. 2021;27:387–413. doi: 10.1016/j.cardfail.2021.01.022 - DOI - PubMed
-
- Tsao CW, Aday AW, Almarzooq ZI, Anderson CA, Arora P, Avery CL, Baker‐Smith CM, Beaton AZ, Boehme AK, Buxton AE, et al. Heart disease and stroke statistics‐2023 update: a report from the American Heart Association. Circulation. 2023;147:e93–e621. doi: 10.1161/CIR.0000000000001123 - DOI - PMC - PubMed
-
- Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM, Deswal A, Drazner MH, Dunlay SM, Evers LR, et al. 2022 AHA/ACC/HFSA guideline for the management of heart failure: executive summary: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2022;145:e876–e894. doi: 10.1161/CIR.0000000000001062 - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
