

Effectiveness of Colonoscopy Screening vs Sigmoidoscopy Screening in Colorectal Cancer
- PMID: 38421651
- PMCID: PMC10905314
- DOI: 10.1001/jamanetworkopen.2024.0007
Effectiveness of Colonoscopy Screening vs Sigmoidoscopy Screening in Colorectal Cancer
Abstract
Importance: Randomized clinical screening trials have shown that sigmoidoscopy screening reduces colorectal cancer (CRC) incidence and mortality. Colonoscopy has largely replaced sigmoidoscopy for CRC screening, but long-term results from randomized trials on colonoscopy screening are still lacking.
Objective: To estimate the additional screening benefit of colonoscopy compared with sigmoidoscopy.
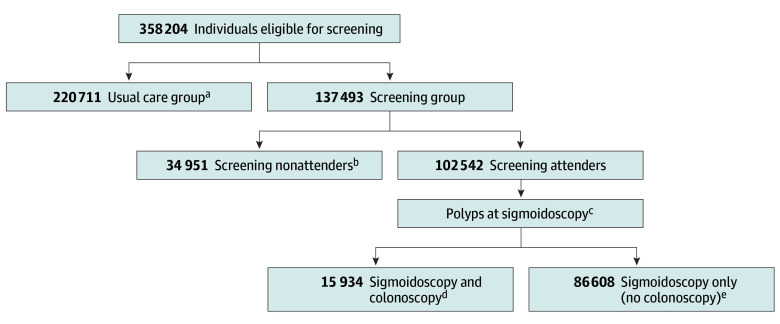
Design, setting, and participants: This comparative effectiveness simulation study pooled data on 358 204 men and women randomly assigned to sigmoidoscopy screening or usual care in 4 randomized sigmoidoscopy screening trials conducted in Norway, Italy, the US, and UK with inclusion periods in the years 1993 to 2001. The primary analysis of the study was conducted from January 19 to December 30, 2021.
Intervention: Invitation to endoscopic screening.
Main outcomes and measures: Primary outcomes were CRC incidence and mortality. Using pooled 15-year follow-up data, colonoscopy screening effectiveness was estimated assuming that the efficacy of colonoscopy in the proximal colon was similar to that observed in the distal colon in the sigmoidoscopy screening trials. The simulation model was validated using data from Norwegian participants in a colonoscopy screening trial.
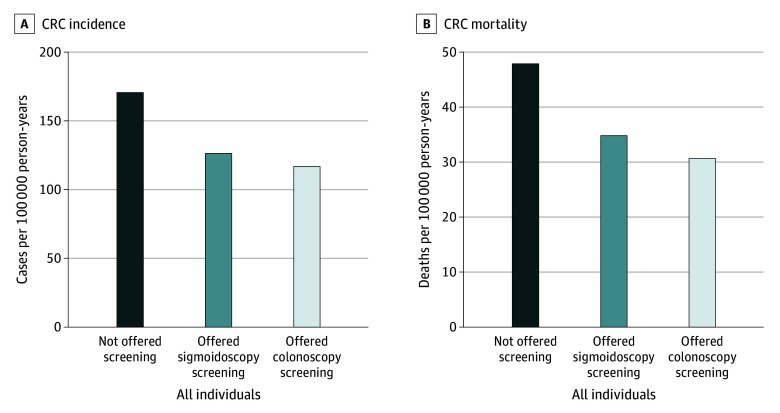
Results: This analysis included 358 204 individuals (181 971 women [51%]) aged 55 to 64 years at inclusion with a median follow-up time ranging from 15 to 17 years. Compared with usual care, colonoscopy prevented an estimated 50 (95% CI, 42-58) CRC cases per 100 000 person-years, corresponding to 30% incidence reduction (rate ratio, 0.70 [95% CI, 0.66-0.75]), and prevented an estimated 15 (95% CI, 11-19) CRC deaths per 100 000 person-years, corresponding to 32% mortality reduction (rate ratio, 0.68 [95% CI, 0.61-0.76]). The additional benefit of colonoscopy screening compared with sigmoidoscopy was 12 (95% CI, 10-14) fewer CRC cases and 4 (95% CI, 3-5) fewer CRC deaths per 100 000 person-years, corresponding to percentage point reductions of 6.9 (95% CI, 6.0-7.9) for CRC incidence and 7.6 (95% CI, 5.7-9.6) for CRC mortality. The number needed to switch from sigmoidoscopy to colonoscopy screening was 560 (95% CI, 486-661) to prevent 1 CRC case and 1611 (95% CI, 1275-2188) to prevent 1 CRC death.
Conclusions and relevance: The findings of this comparative effectiveness study assessing long-term follow-up after CRC screening suggest that there was an additional preventive effect on CRC incidence and mortality associated with colonoscopy screening compared with sigmoidoscopy screening, but the additional preventive effect was less than what was achieved by introducing sigmoidoscopy screening where no screening existed. The results probably represent the upper limit of what may be achieved with colonoscopy screening compared with sigmoidoscopy screening.
Conflict of interest statement
Figures
References
-
- Miller EA, Pinsky PF, Schoen RE, Prorok PC, Church TR. Effect of flexible sigmoidoscopy screening on colorectal cancer incidence and mortality: long-term follow-up of the randomised US PLCO cancer screening trial. Lancet Gastroenterol Hepatol. 2019;4(2):101-110. doi:10.1016/S2468-1253(18)30358-3 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
