

Aging and comprehensive molecular profiling in acute myeloid leukemia
- PMID: 38422020
- PMCID: PMC10927507
- DOI: 10.1073/pnas.2319366121
Aging and comprehensive molecular profiling in acute myeloid leukemia
Abstract
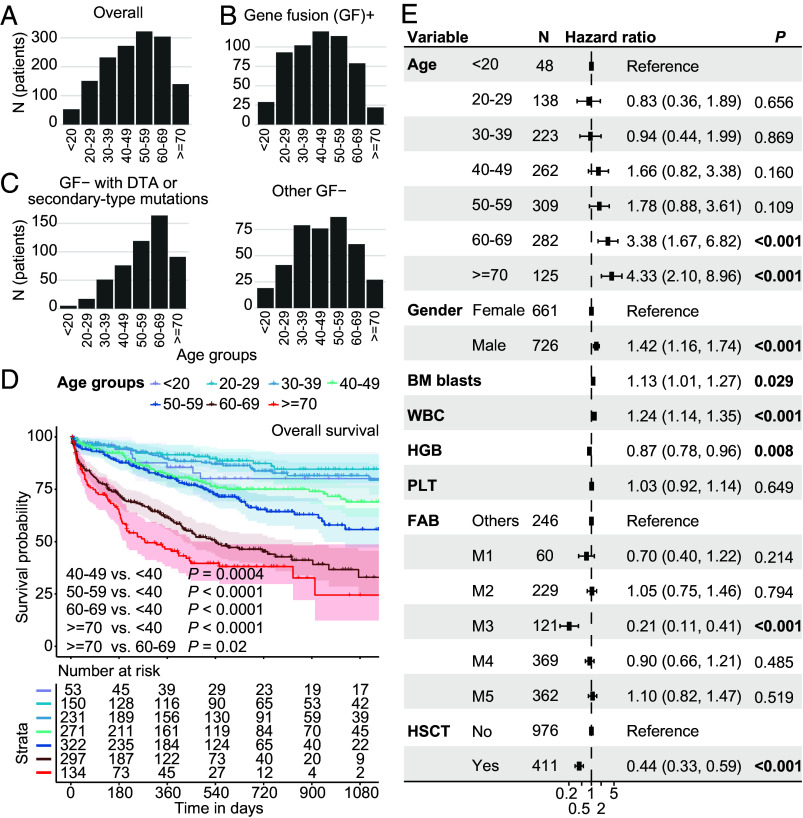
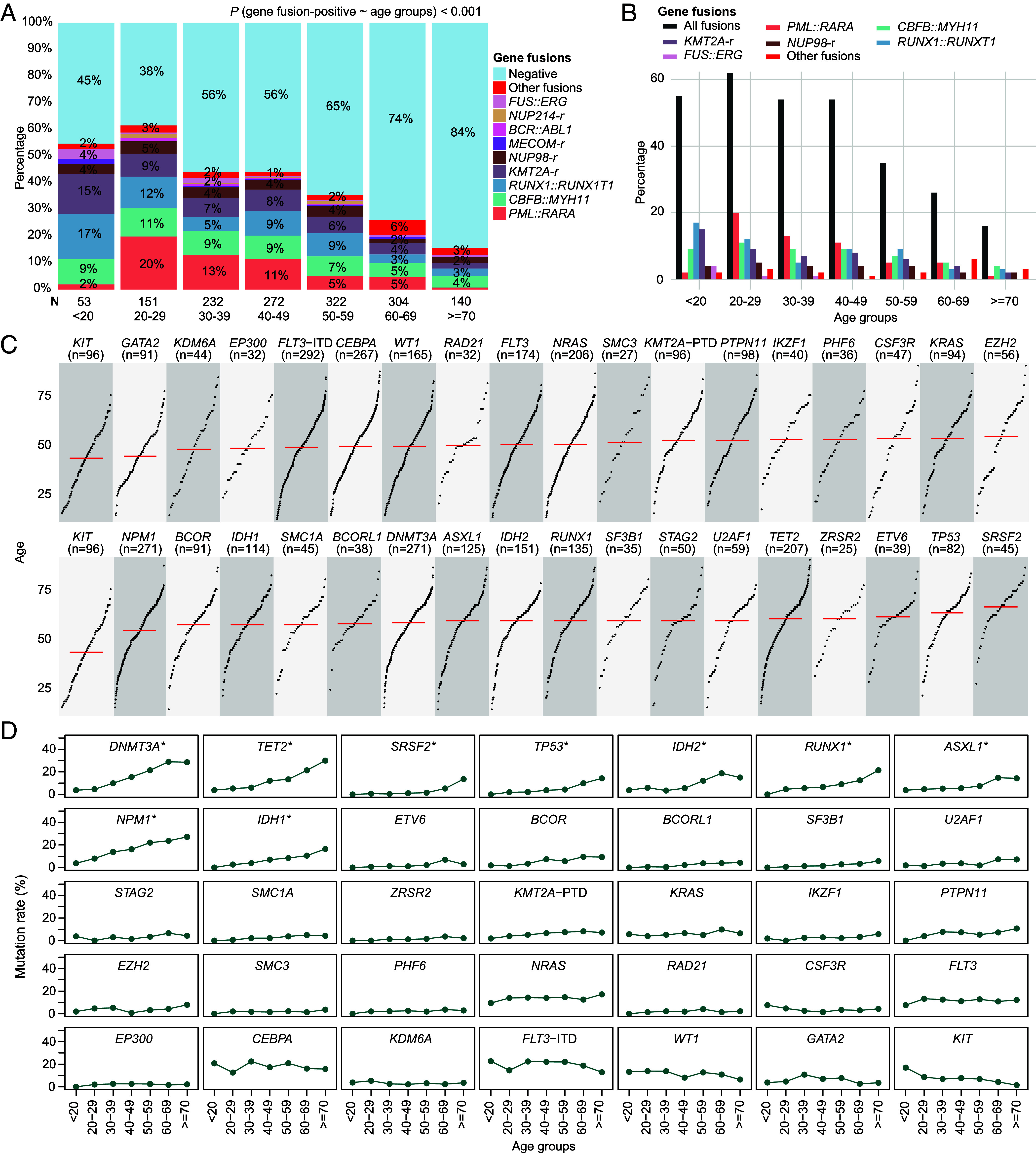
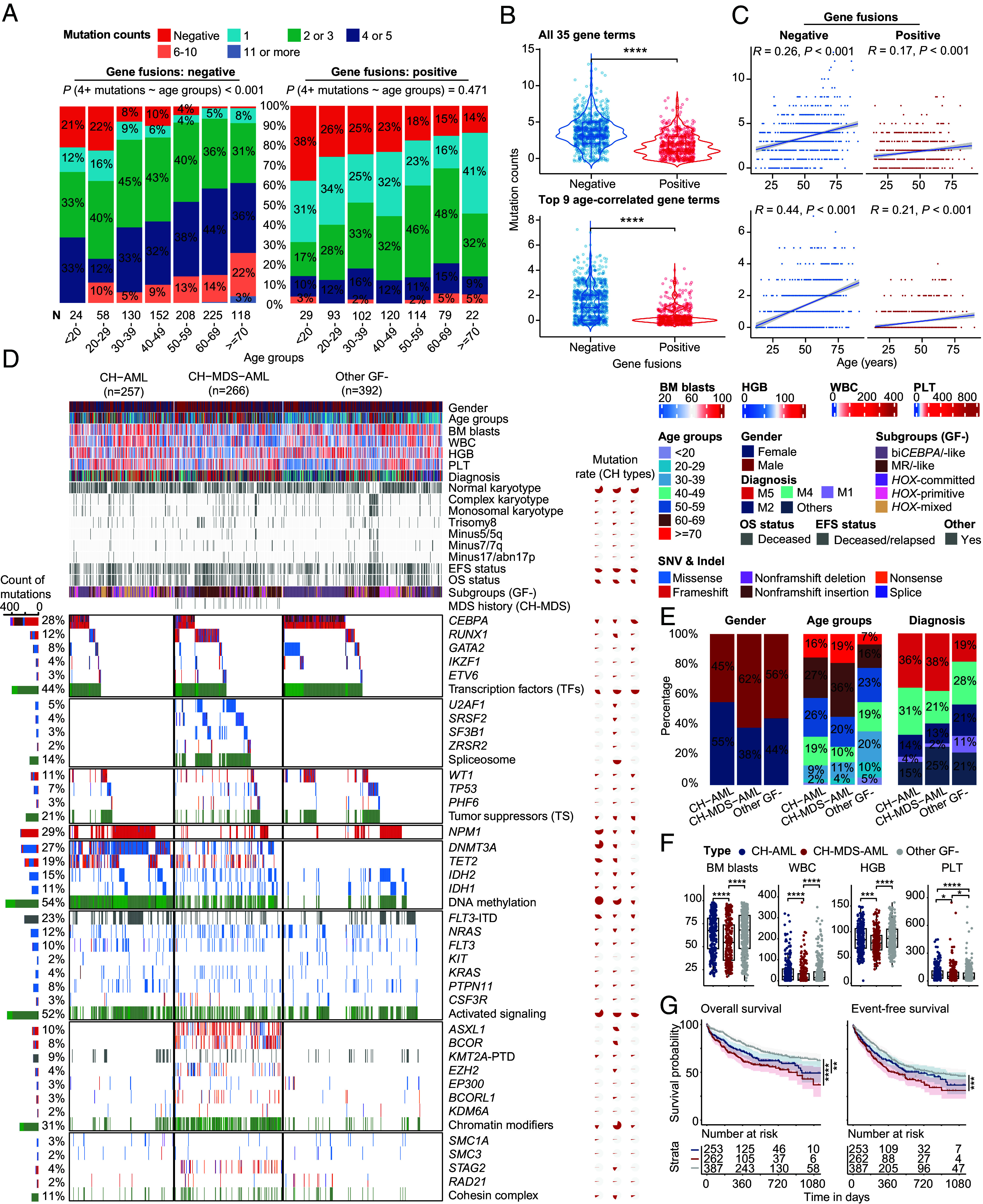
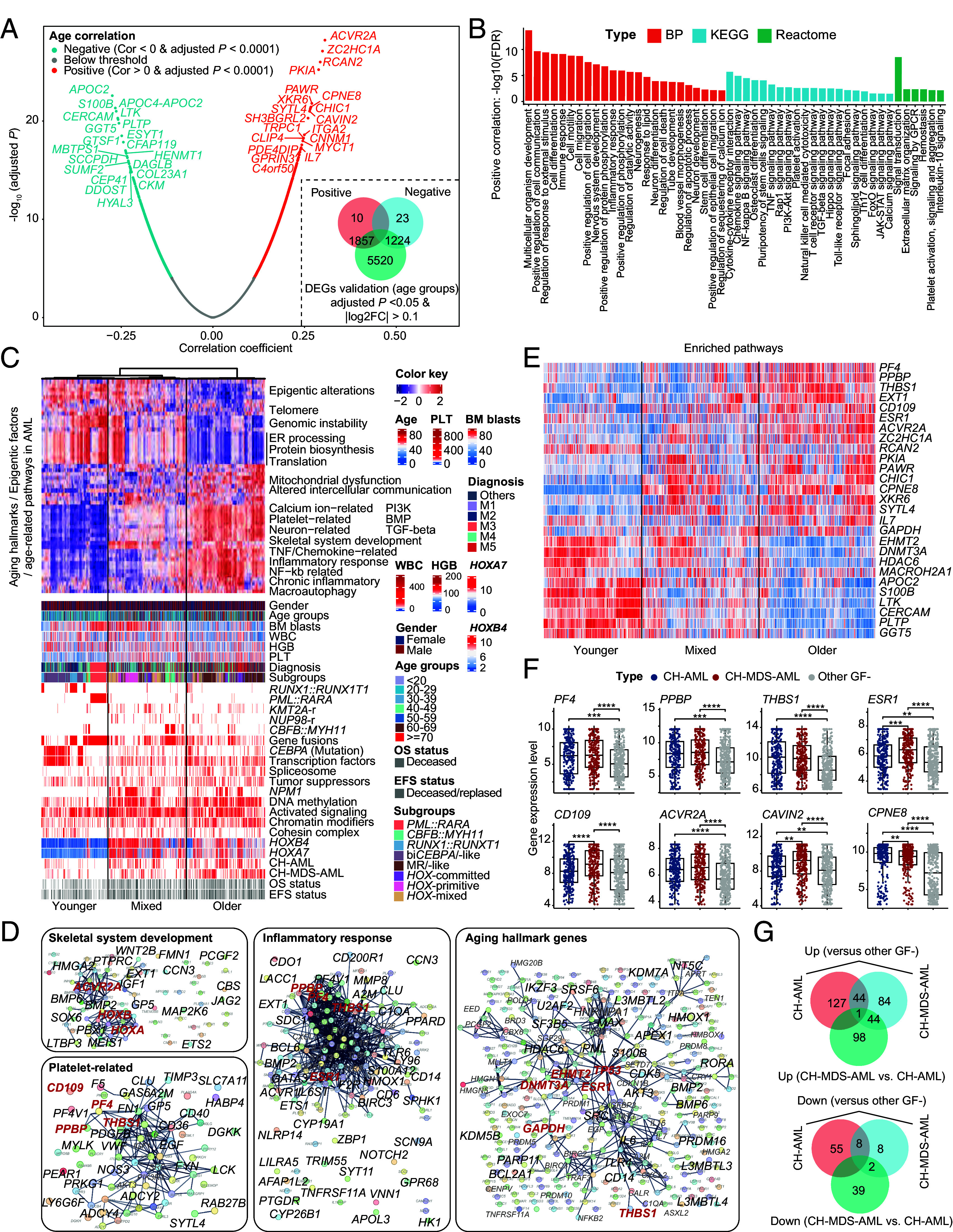
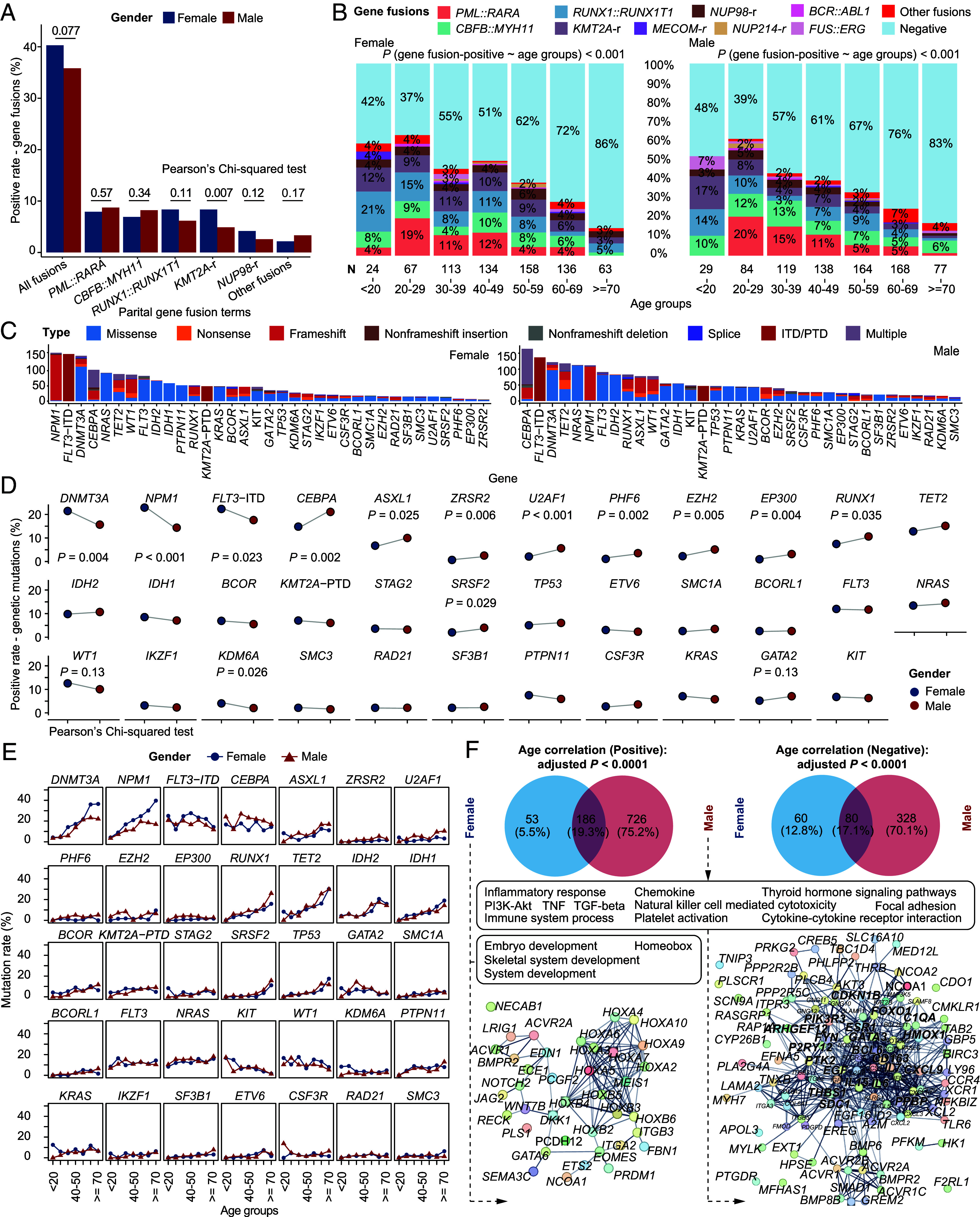
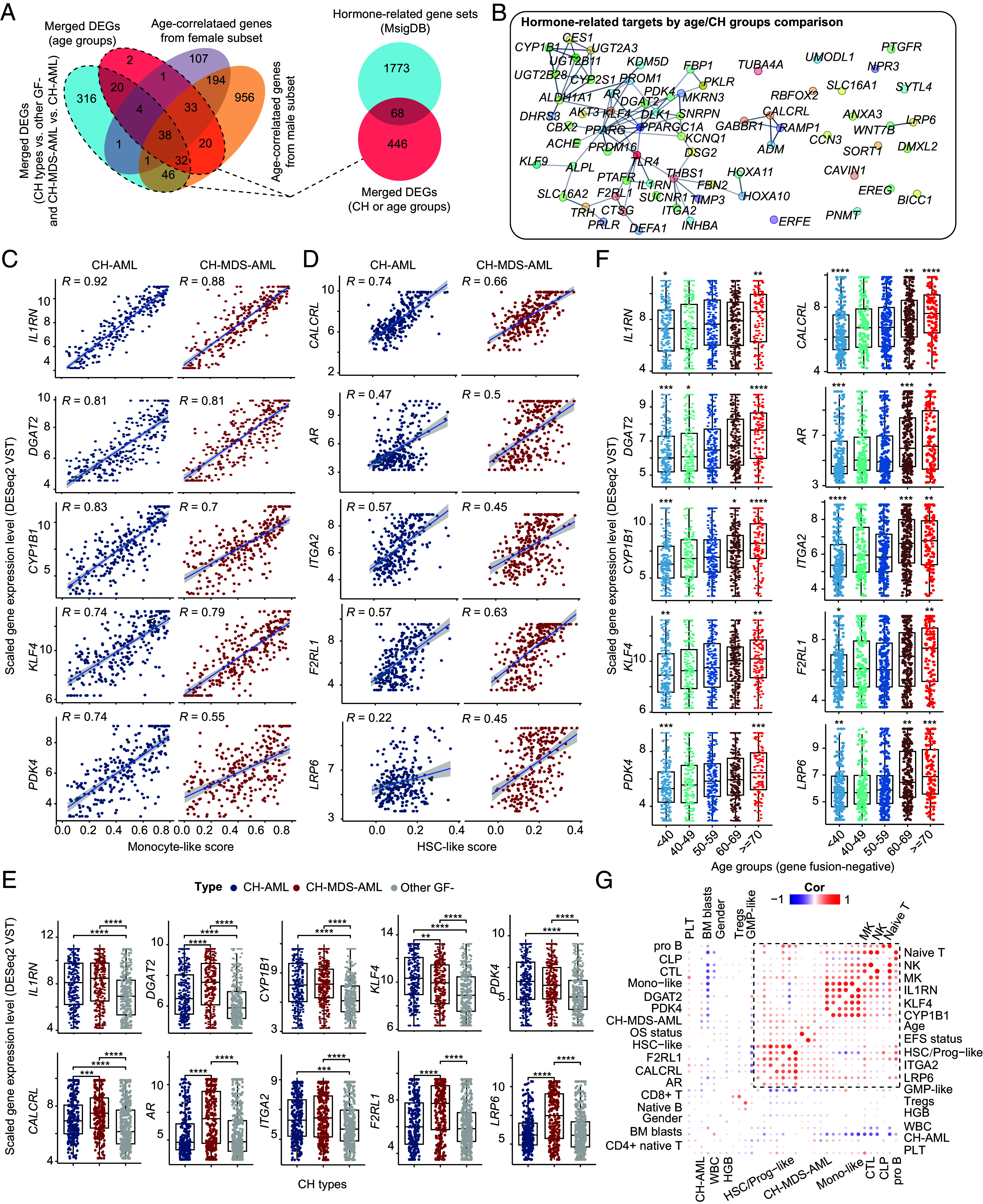
Acute myeloid leukemia (AML) is an aging-related and heterogeneous hematopoietic malignancy. In this study, a total of 1,474 newly diagnosed AML patients with RNA sequencing data were enrolled, and targeted or whole exome sequencing data were obtained in 94% cases. The correlation of aging-related factors including age and clonal hematopoiesis (CH), gender, and genomic/transcriptomic profiles (gene fusions, genetic mutations, and gene expression networks or pathways) was systematically analyzed. Overall, AML patients aged 60 y and older showed an apparently dismal prognosis. Alongside age, the frequency of gene fusions defined in the World Health Organization classification decreased, while the positive rate of gene mutations, especially CH-related ones, increased. Additionally, the number of genetic mutations was higher in gene fusion-negative (GF-) patients than those with GF. Based on the status of CH- and myelodysplastic syndromes (MDS)-related mutations, three mutant subgroups were identified among the GF- AML cohort, namely, CH-AML, CH-MDS-AML, and other GF- AML. Notably, CH-MDS-AML demonstrated a predominance of elderly and male cases, cytopenia, and significantly adverse clinical outcomes. Besides, gene expression networks including HOXA/B, platelet factors, and inflammatory responses were most striking features associated with aging and poor prognosis in AML. Our work has thus unraveled the intricate regulatory circuitry of interactions among different age, gender, and molecular groups of AML.
Keywords: RNA-seq; acute myeloid leukemia; aging; clonal hematopoiesis; molecular alterations.
Conflict of interest statement
Competing interests statement:The authors declare no competing interest.
Figures
References
-
- Dufva O., et al. , Immunogenomic landscape of hematological malignancies. Cancer Cell 38, 380–399.e13 (2020). - PubMed
-
- Miranda-Filho A., et al. , Epidemiological patterns of leukaemia in 184 countries: A population-based study. Lancet Haematol. 5, e14–e24 (2018). - PubMed
-
- DiNardo C. D., Erba H. P., Freeman S. D., Wei A. H., Acute myeloid leukaemia. Lancet 401, 2073–2086 (2023). - PubMed
-
- Newell L. F., Cook R. J., Advances in acute myeloid leukemia. BMJ 375, n2026 (2021). - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
