

Contribution of proactive management of healthcare risks to the reduction of adverse events in a maternity hospital
- PMID: 38423586
- PMCID: PMC10910639
- DOI: 10.1136/bmjoq-2023-002456
Contribution of proactive management of healthcare risks to the reduction of adverse events in a maternity hospital
Abstract
Background: The risks of the childbirth assistance process are still very high, both for mothers and babies. According to the WHO, birth-related asphyxia accounts for 23% of all 3.3 million annual neonatal deaths and an even larger number of survivors with disabilities. On the other hand, maternal mortality is still a global challenge, affecting 17 mothers per 100 000 births in the USA. This is associated with the use of outdated technologies and a lack of well-defined processes in monitoring labour and early recognition of maternal clinical deterioration.
Method: This study used Lean methodology to map the care flow for pregnant women in a Brazilian maternity hospital (Hospital Israelita Albert Einstein) in order to identify the risks within this process and a set of actions to minimise them. The work team consisted of 29 individuals, including local medical and nursing leaders, as well as healthcare professionals. The What-if tool was used to categorise the levels of risks, and the proportion of severe and catastrophic adverse events was evaluated before and after the implementation of changes.
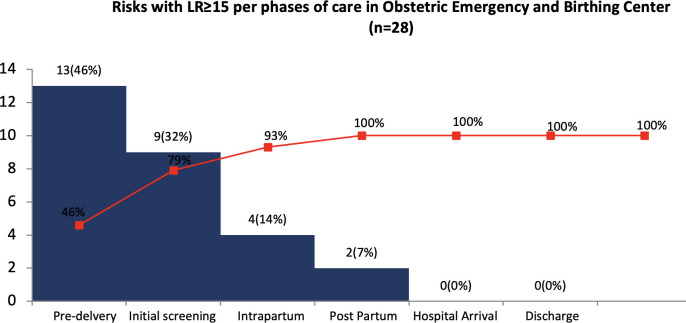
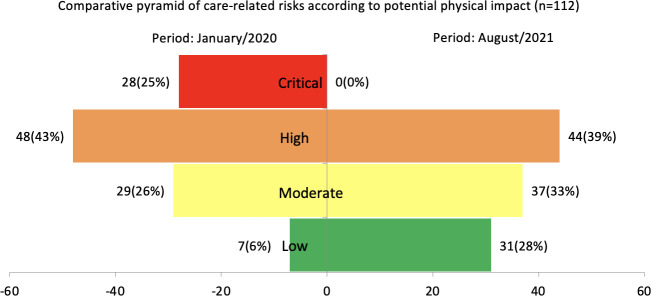
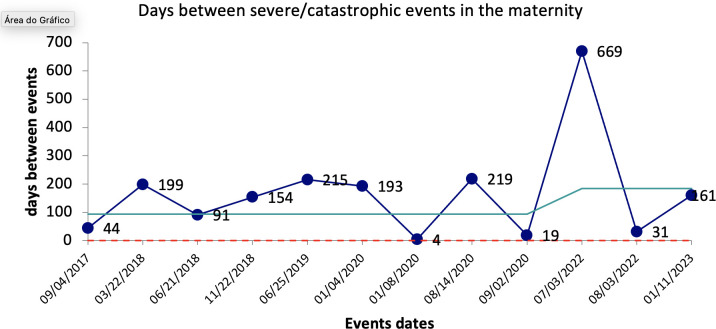
Results: After the implementation of the actions, 100% of the extreme risks (28 risks) and 8% of the high risks (4 risks) were eliminated. This led to a reduction in the interval between severe/catastrophic events from 126 to 284 days, even with an increase in the average monthly number of visits from 367 to 449. Consequently, the weighted value of events decreased from 7.91 to 3.29 per 1000 patients treated, resulting in an annual cost savings of R$693 646.80 (US$139 000.00).
Discussion: The construction of a process based on Lean methodology was essential for mapping the involved risks and implementing a set of actions to minimise them. The participation of the healthcare team and leadership seemed to be important in choosing the measures to be adopted and their applicability. The results found can be attributed to both the established changes and the safety culture brought about by this constructive process.
Keywords: Harm Reduction; Lean management; Obstetrics and gynecology; Patient safety; Risk management.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
The future of Cochrane Neonatal.Early Hum Dev. 2020 Nov;150:105191. doi: 10.1016/j.earlhumdev.2020.105191. Epub 2020 Sep 12. Early Hum Dev. 2020. PMID: 33036834
-
Trends in utilization of obstetric care at Wesley Guild Hospital, Ilesa, Nigeria. Effects of a depressed economy.Trop Geogr Med. 1995;47(2):86-8. Trop Geogr Med. 1995. PMID: 8592770
-
Adverse obstetric outcomes in two Brazilian maternity hospitals.Int J Health Care Qual Assur. 2021 Jan 5;ahead-of-print(ahead-of-print). doi: 10.1108/IJHCQA-02-2020-0026. Int J Health Care Qual Assur. 2021. PMID: 33393747
-
Breastfeeding promotion and priority setting in health.Health Policy Plan. 1996 Jun;11(2):156-68. doi: 10.1093/heapol/11.2.156. Health Policy Plan. 1996. PMID: 10158457 Review.
-
Reduction of maternal and perinatal mortality in rural and peri-urban settings: what works?Eur J Obstet Gynecol Reprod Biol. 1996 Oct;69(1):47-53. doi: 10.1016/0301-2115(95)02535-9. Eur J Obstet Gynecol Reprod Biol. 1996. PMID: 8909956 Review.
References
-
- Institute of Medicine . To err is human: building a safer health system. Washington: National Academy Press; 1999.
-
- Federico F. Is your organization highly reliable. Healthc Exec 2018;33:76–9. 10.1017/9781108601993 Available: https://www.ihi.org/sites/default/files/Federico_IsYourOrganizationHighl... - DOI
-
- Abate BB, Bimerew M, Gebremichael B, et al. . Effects of therapeutic hypothermia on death among asphyxiated neonates with hypoxic- ischemic encephalopathy: a systematic review and meta-analysis of randomized control trials. PLoS One 2021;16:e0247229. 10.1371/journal.pone.0247229 - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical