

Implementation of an enhanced recovery after surgery protocol for colorectal cancer in a regional hospital network supported by audit and feedback: a stepped wedge, cluster randomised trial
- PMID: 38423752
- PMCID: PMC11103294
- DOI: 10.1136/bmjqs-2023-016594
Implementation of an enhanced recovery after surgery protocol for colorectal cancer in a regional hospital network supported by audit and feedback: a stepped wedge, cluster randomised trial
Abstract
Background: Enhanced recovery after surgery (ERAS) protocols are known to potentially improve the management and outcomes of patients undergoing colorectal surgery, with limited evidence of their implementation in hospital networks and in a large population. We aimed to assess the impact of the implementation of an ERAS protocol in colorectal cancer surgery in the entire region of Piemonte, Italy, supported by an audit and feedback (A&F) intervention.
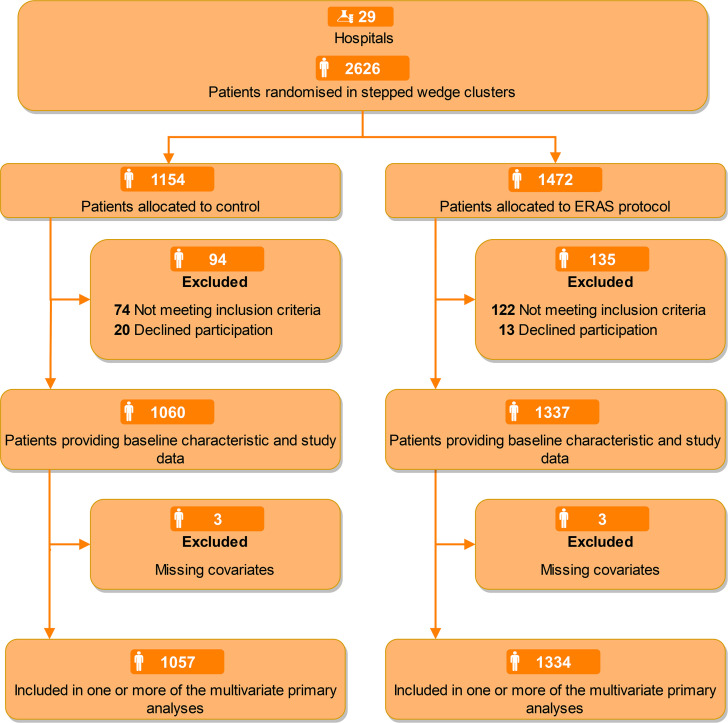
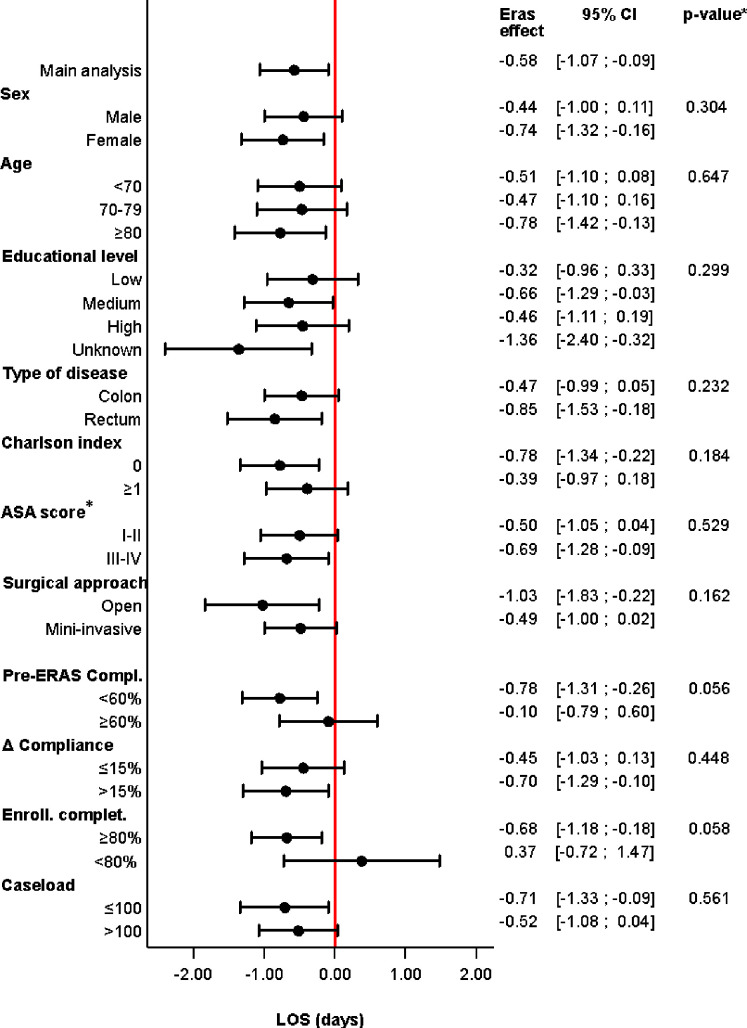
Methods: A large, stepped wedge, cluster randomised trial enrolled patients scheduled for elective surgery at 29 general surgery units (clusters). At baseline (first 3 months), standard care was continued in all units. Thereafter, four groups of clusters began to adopt the ERAS protocol successively. By the end of the study, each cluster had a period in which standard care was maintained (control) and a period in which the protocol was applied (experimental). ERAS implementation was supported by initial training and A&F initiatives. The primary endpoint was length of stay (LOS) without outliers (>94th percentile), and the secondary endpoints were outliers for LOS, postoperative medical and surgical complications, quality of recovery and compliance with ERAS items.
Results: Of 2626 randomised patients, 2397 were included in the LOS analysis (1060 in the control period and 1337 in the experimental period). The mean LOS without outliers was 8.5 days during the control period (SD 3.9) and 7.5 (SD 3.5) during the experimental one. The adjusted difference between the two periods was a reduction of -0.58 days (95% CI -1.07, -0.09; p=0.021). The compliance with ERAS items increased from 52.4% to 67.3% (estimated absolute difference +13%; 95% CI 11.4%, 14.7%). No difference in the occurrence of complications was evidenced (OR 1.22; 95% CI 0.89, 1.68).
Conclusion: Implementation of the ERAS protocol for colorectal cancer, supported by A&F approach, led to a substantial improvement in compliance and a reduction in LOS, without meaningful effects on complications. Trial registration number NCT04037787.
Keywords: Audit and feedback; Quality improvement; Surgery.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical