

The impact of GLP-1 receptor agonist liraglutide on blood pressure profile, hydration, natriuresis in diabetic patients with severely impaired kidney function
- PMID: 38424466
- PMCID: PMC10904847
- DOI: 10.1038/s41598-024-55724-z
The impact of GLP-1 receptor agonist liraglutide on blood pressure profile, hydration, natriuresis in diabetic patients with severely impaired kidney function
Abstract
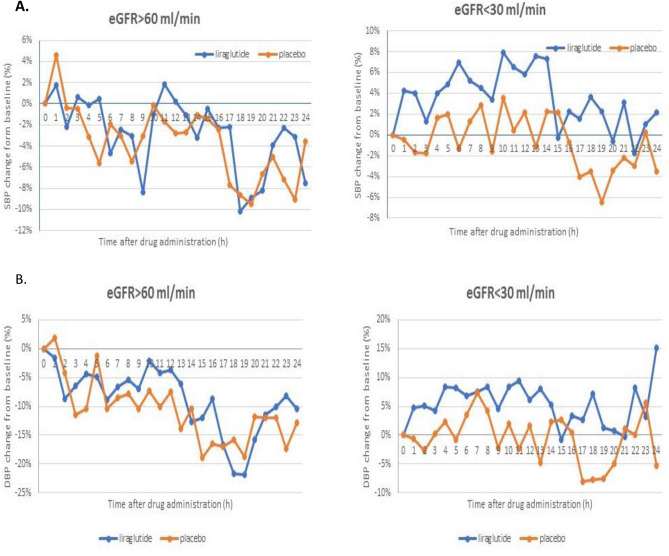
Chronic treatment with GLP-1R agonists may moderately lower blood pressure due to increased natriuresis and RAAS inhibition. Short-term effect of these drugs on blood pressure may be opposite and its mechanism remains unclear. We investigated the effect of a single dose of liraglutide on diurnal blood pressure profile, natriuresis, hydration and serum concentration of renin, aldosterone and atrial natriuretic peptide (ANP) in diabetic kidney disease (DKD). 17 patients with eGFR < 30 ml/min/1.73 m2 and 17 with > 60 ml/min/1.73 m2 received in a random order a single subcutaneous dose 1.2 mg liraglutide and placebo with subsequent 24 h blood pressure and natriuresis monitoring. Before and after each medication thoracic fluid index and plasma renin, aldosterone and ANP were also assessed. The blood pressure load in the daytime and nighttime were significantly increased after liraglutide compared to placebo in patients with eGFR < 30 ml/min/1.73 m2. In patients with eGFR > 60 ml/min/1.73 m2 the changes of arterial pressure were comparable, while the morning surge was significantly reduced after liraglutide compared to placebo. After liraglutide 24 h urine sodium excretion increased in both groups vs. placebo (p < 0.001), the effect was greatest in subjects with eGFR > 60 ml/min/1.73 m2. Plasma ANP increased after liraglutide in both groups, most in patients with eGFR < 30 ml/min/1.73 m2 group. Plasma aldosterone (p = 0.013) and thoracic fluid index (p = 0.01) decreased after liraglutide compared to placebo (p = 0.013 and p + 0.01, respectively. Plasma renin concentration remained unchanged. In severe chronic kidney disease liraglutide induces a transient increase of blood pressure due to reduced natriuresis. The natriuretic effect of liraglutide in DKD may be related to increased ANP and decreased aldosterone secretion.
Keywords: Blood pressure; Diabetic kidney disease; Liraglutide; Natriuresis; Renin–angiotensin–aldosterone system.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
