

Postoperative epidural hematoma as a rare complication after intracranial tumor resection: a case series report and causes analysis
- PMID: 38424654
- PMCID: PMC10905794
- DOI: 10.1186/s41016-024-00359-2
Postoperative epidural hematoma as a rare complication after intracranial tumor resection: a case series report and causes analysis
Abstract
Background: To review the treatment and the causes of postoperative epidural hematoma (PEDH) after intracranial tumor resection.
Method: A retrospective case study was conducted to examine a series of patients who developed PEDH as a complication following intracranial tumor resection between January 2016 and June 2021. The study collected data from hospital charts, including clinical status at admission, imaging results, histopathologic findings, surgical management, complications, and outcomes. Causes of PEDH were evaluated through a review of operative notes and discussions with the surgical team.
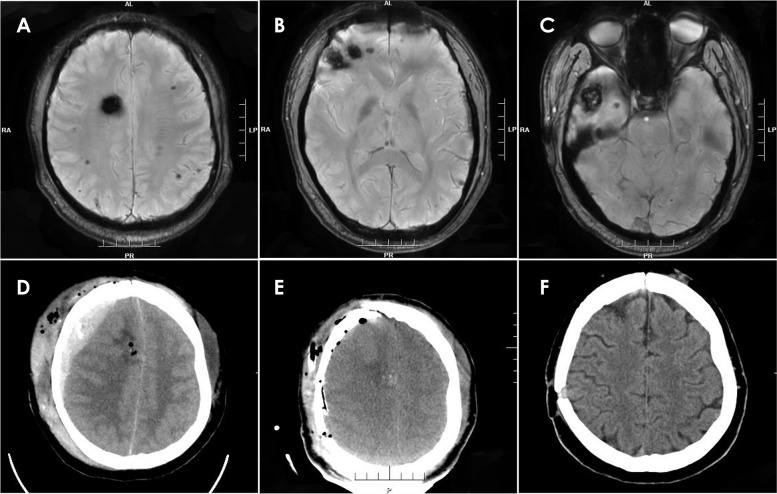
Results: Twenty-five patients (10 males, 15 females; median age 42 years, range 11-61 years; median medical history 27 months, range 1-96 months) were enrolled in the study. Regarding tumor location, 16 cases exhibited supratentorial brain tumors, 4 cases had infratentorial brain tumors, 2 cases of tumors occurred in the petroclival region, 2 cases in the peritorcular region, and 1 case in the pineal region. Four of these cases were complicated with supratentorial hydrocephalus. The 25 cases in this study were classified into four types based on location. Type 1 refers to EDHs that occur at the adjacent site of the operative field without involvement of the surgical area. Type 2 includes hematomas that occur at the adjacent site of the surgical area and the surgical area. Type 3 includes EDHs that occur in distant areas, and type 4 involves EDHs in the surgical field. The numbers of cases of types 1, 2, 3, and 4 PEDHs were 16, 2, 3, and 4 cases, respectively. Most PEDHs were associated with reduced ICP after craniotomy due to intracranial tumor resection and substantial loss of CSF. All patients achieved satisfactory outcomes after hematoma evacuation.
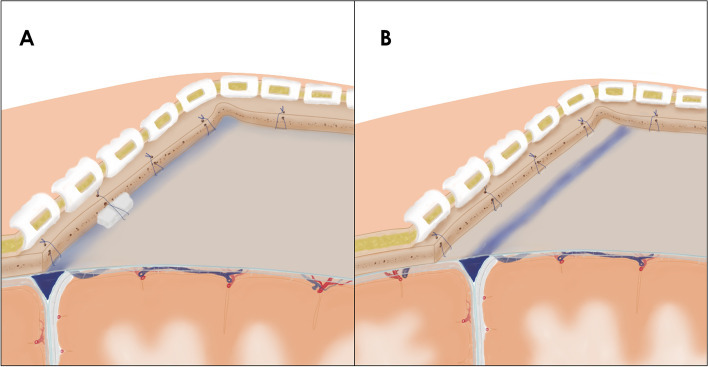
Conclusion: The decrease in ICP resulting from intracranial tumor resection and CSF loss might lead to PEDHs. By employing optimized surgical techniques and meticulous patient management to prevent rapid decreases in ICP and dural detachment, we can potentially lower the incidence of PEDHs. Additionally, prompt evacuation of hematomas can contribute to positive outcomes.
Keywords: Brain tumor; Craniotomy; Epidural hematoma; Postoperative complication.
© 2024. The Author(s).
Conflict of interest statement
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Figures





Similar articles
-
Retrospective analysis of 14 cases of remote epidural hematoma as a postoperative complication after intracranial tumor resection.World J Surg Oncol. 2016 Jan 6;14(1):1. doi: 10.1186/s12957-015-0754-8. World J Surg Oncol. 2016. PMID: 26732900 Free PMC article.
-
Multiple Remote Sequential Supratentorial Epidural Hematomas-An Unusual and Rare Complication After Posterior Fossa Surgery.World Neurosurg. 2019 Aug;128:83-90. doi: 10.1016/j.wneu.2019.04.228. Epub 2019 May 6. World Neurosurg. 2019. PMID: 31071445
-
Surgical Closed Suction Drain Use After Craniotomy for Evacuation of Supratentorial Epidural Hematomas: A Case Series of Radiographic and Clinical Outcomes.World Neurosurg. 2020 Feb;134:e460-e468. doi: 10.1016/j.wneu.2019.10.098. Epub 2019 Oct 24. World Neurosurg. 2020. PMID: 31669243
-
Acute intracranial hematoma formation following excision of a cervical subdural tumor: a report of two cases and literature review.Br J Neurosurg. 2014 Jan;28(1):125-30. doi: 10.3109/02688697.2013.815316. Epub 2013 Jul 12. Br J Neurosurg. 2014. PMID: 23848602 Review.
-
Postoperative spinal epidural hematoma at a site distant from the main surgical procedure: a case report and review of the literature.Spine J. 2010 Apr;10(4):e21-5. doi: 10.1016/j.spinee.2010.02.011. Spine J. 2010. PMID: 20362244 Review.
References
LinkOut - more resources
Full Text Sources