

A case report of multicentric reticulohistiocytosis with atypical cutaneous presentation
- PMID: 38426104
- PMCID: PMC10903083
- DOI: 10.3389/fimmu.2024.1344313
A case report of multicentric reticulohistiocytosis with atypical cutaneous presentation
Abstract
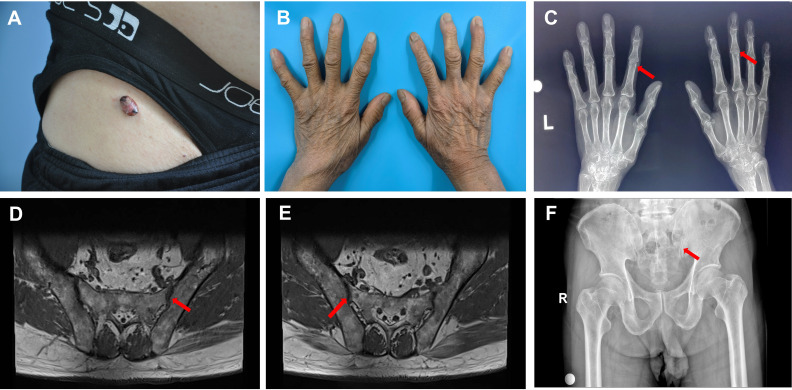
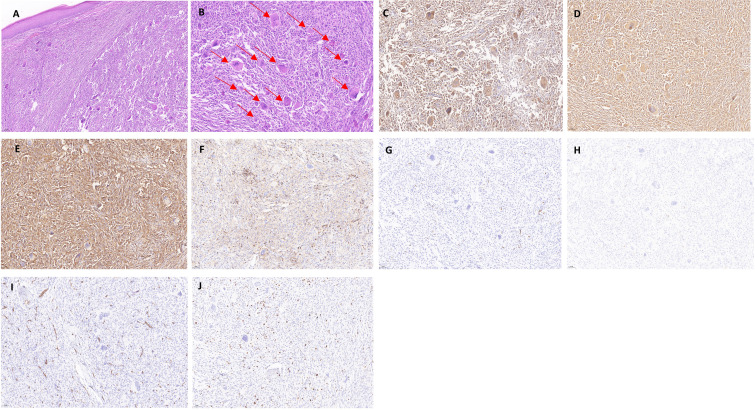
Multicentric reticulohistiocytosis (MRH) is a rare systemic disorder characterized by histiocytic hyperplasia that mainly involves the skin, mucous membranes, and joints. The typical clinical features include papules, nodules, and arthritis. MRH lesions are relatively extensive but small and scattered. Joint inflammation is characterized by diffuse symmetric polyarthritis as the first symptom, which can be severe and disabling due to destructive joint changes. MRH is easily misdiagnosed in clinical practice. Here, we report the case of an elderly male patient who presented with polyarticular pain in the hip and interphalangeal joints as the first manifestation, followed by the development of large, isolated, bulging skin nodules, which are atypical MRH lesions. This is rare in all MRH case reports, and we made the correct diagnosis by combining skin histopathology, immunohistochemistry, and other clinical examinations. We performed surgical treatment on the local skin lesions of this patient. This case suggests that clinicians should actively correlate the condition and accurately diagnose MRH when encountering atypical skin changes or other diseases as the first symptom and explore the mechanisms of MRH and other clinical manifestations.
Keywords: differential diagnosis; gouty arthritis; immunohistochemistry; multicentric reticulohistiocytosis; nodular xanthomatosis.
Copyright © 2024 Chen, An, Jiang and Jia.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

Similar articles
-
A case of multicentric reticulohistiocytosis.Mod Rheumatol. 2017 Jan;27(1):165-168. doi: 10.3109/14397595.2014.952702. Epub 2014 Sep 11. Mod Rheumatol. 2017. PMID: 25211404
-
Clinical characteristics of multicentric reticulohistiocytosis and distinguished features from rheumatoid arthritis: a single-center experience in China.Orphanet J Rare Dis. 2022 Apr 12;17(1):164. doi: 10.1186/s13023-022-02311-y. Orphanet J Rare Dis. 2022. PMID: 35413870 Free PMC article.
-
Multicentric Reticulohistiocytosis (Mrh): A Case Report On A Rare Destructive Arthritis.J Ayub Med Coll Abbottabad. 2023 Apr-Jun;35(2):316-319. doi: 10.55519/JAMC-02-9261. J Ayub Med Coll Abbottabad. 2023. PMID: 37422829
-
Multicentric reticulohistiocytosis presenting with papulonodular skin eruption and polyarthritis.Eur J Dermatol. 2005 May-Jun;15(3):196-200. Eur J Dermatol. 2005. PMID: 15908308 Review.
-
Multicentric Reticulohistiocytosis Associated with an Early Form of Systemic Lupus Erythematosus: A Case Report of a Rare Disease, with Mini Review of the Literature.J Clin Med. 2022 Nov 3;11(21):6529. doi: 10.3390/jcm11216529. J Clin Med. 2022. PMID: 36362761 Free PMC article. Review.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical