

The etiologies of Kawasaki disease
- PMID: 38426498
- PMCID: PMC10904046
- DOI: 10.1172/JCI176938
The etiologies of Kawasaki disease
Abstract
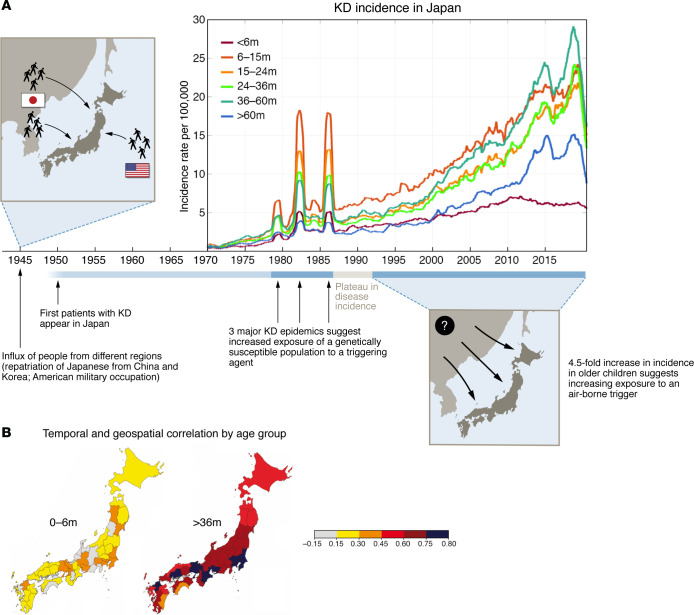
Kawasaki disease (KD) is a systemic vasculitis that affects young children and can result in coronary artery aneurysms. The etiology is currently unknown, but new clues from the epidemiology of KD in Japan, the country of highest incidence, are beginning to shed light on what may trigger this acute inflammatory condition. Additional clues from the global changes in KD incidence during the COVID-19 pandemic, coupled with a new birth cohort study from Japan, point to the potential role of person-to-person transmission of an infectious agent. However, the rising incidence of KD in Japan, with coherent waves across the entire country, points to an increasing intensity of exposure that cannot be explained by person-to-person spread. This Review discusses new and historical observations that guide us toward a better understanding of KD etiology and explores hypotheses and interpretations that can provide direction for future investigations. Once the etiology of KD is determined, accurate diagnostic tests will become available, and new, less expensive, and more effective targeted therapies will likely be possible. Clearly, solving the mystery of the etiologies of KD remains a priority for pediatric research.
Conflict of interest statement
Figures



Similar articles
-
Kawasaki disease: A brief history.Pediatrics. 2000 Aug;106(2):E27. doi: 10.1542/peds.106.2.e27. Pediatrics. 2000. PMID: 10920183 Review.
-
Incidence of Kawasaki disease before and during the COVID-19 pandemic: a retrospective cohort study in Japan.BMJ Paediatr Open. 2021 Apr 2;5(1):e001034. doi: 10.1136/bmjpo-2021-001034. eCollection 2021. BMJ Paediatr Open. 2021. PMID: 33884312 Free PMC article.
-
Epidemiological and Clinical Features of Kawasaki Disease During the COVID-19 Pandemic in the United States.JAMA Netw Open. 2022 Jun 1;5(6):e2217436. doi: 10.1001/jamanetworkopen.2022.17436. JAMA Netw Open. 2022. PMID: 35713905 Free PMC article.
-
Resurgence of Kawasaki Disease Following Relaxation of Coronavirus Disease 2019 Pandemic Restrictions in Japan.J Pediatr. 2024 Dec;275:114251. doi: 10.1016/j.jpeds.2024.114251. Epub 2024 Aug 22. J Pediatr. 2024. PMID: 39181319
-
Kawasaki disease and the environment: an enigmatic interplay.Front Immunol. 2023 Dec 18;14:1259094. doi: 10.3389/fimmu.2023.1259094. eCollection 2023. Front Immunol. 2023. PMID: 38164136 Free PMC article. Review.
Cited by
-
Unraveling the gut: the pivotal role of intestinal mechanisms in Kawasaki disease pathogenesis.Front Immunol. 2024 Nov 26;15:1496293. doi: 10.3389/fimmu.2024.1496293. eCollection 2024. Front Immunol. 2024. PMID: 39664384 Free PMC article. Review.
-
Identification of a mimotope of a complex gp41 Human Immunodeficiency VIrus epitope related to a non-structural protein of Hepacivirus previously implicated in Kawasaki disease.bioRxiv [Preprint]. 2024 Jun 28:2024.06.26.600771. doi: 10.1101/2024.06.26.600771. bioRxiv. 2024. Update in: Microbiol Spectr. 2025 Mar 31:e0191124. doi: 10.1128/spectrum.01911-24. PMID: 38979252 Free PMC article. Updated. Preprint.
-
Gut dysbiosis mediates the association between antibiotic exposure and chronic disease.Front Med (Lausanne). 2024 Nov 6;11:1477882. doi: 10.3389/fmed.2024.1477882. eCollection 2024. Front Med (Lausanne). 2024. PMID: 39568738 Free PMC article. Review.
-
Establishment and validation of a nomogram for coronary artery lesions in children with Kawasaki disease.Front Cardiovasc Med. 2025 Jan 14;11:1522473. doi: 10.3389/fcvm.2024.1522473. eCollection 2024. Front Cardiovasc Med. 2025. PMID: 39877016 Free PMC article.
-
Gut microbiota, inflammatory cytokines, and Kawasaki disease: a Mendelian randomization study and mediation analysis.Pediatr Res. 2025 Feb 10. doi: 10.1038/s41390-025-03911-7. Online ahead of print. Pediatr Res. 2025. PMID: 39930249
