

Reduced control of SARS-CoV-2 infection associates with lower mucosal antibody responses in pregnancy
- PMID: 38426787
- PMCID: PMC10964408
- DOI: 10.1128/msphere.00812-23
Reduced control of SARS-CoV-2 infection associates with lower mucosal antibody responses in pregnancy
Abstract
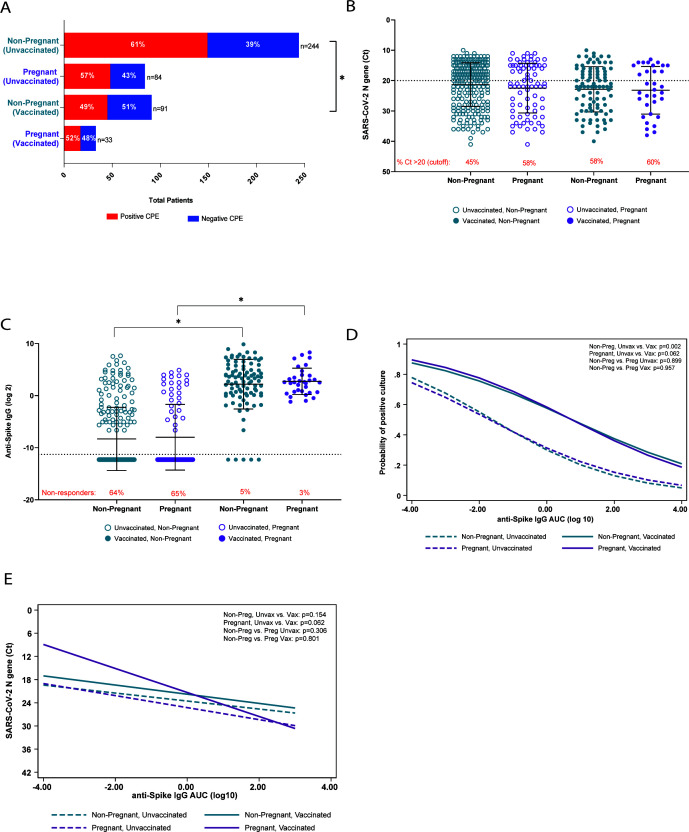
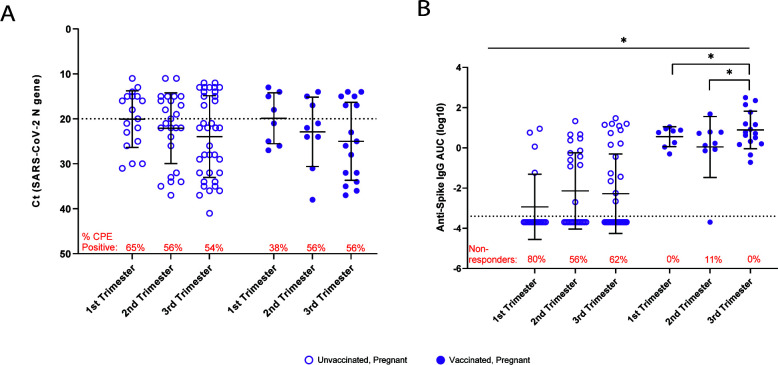
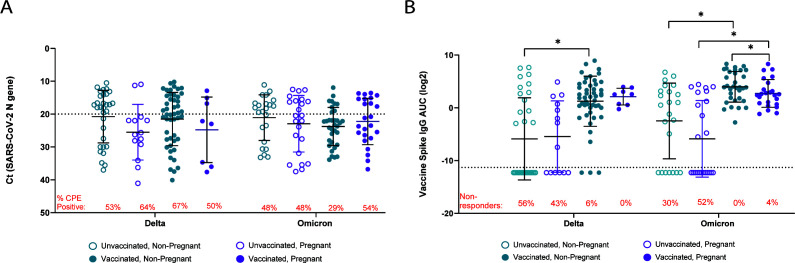
Pregnant patients are at greater risk of hospitalization with severe COVID-19 than non-pregnant people. This was a retrospective observational cohort study of remnant clinical specimens from patients who visited acute care hospitals within the Johns Hopkins Health System in the Baltimore, MD-Washington DC, area between October 2020 and May 2022. Participants included confirmed severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)-infected pregnant people and matched non-pregnant people (the matching criteria included age, race/ethnicity, area deprivation index, insurance status, and vaccination status to ensure matched demographics). The primary dependent measures were clinical COVID-19 outcomes, infectious virus recovery, viral RNA levels, and mucosal anti-spike (S) IgG titers from upper respiratory tract samples. A total of 452 individuals (117 pregnant and 335 non-pregnant) were included in the study, with both vaccinated and unvaccinated individuals represented. Pregnant patients were at increased risk of hospitalization (odds ratio [OR] = 4.2; confidence interval [CI] = 2.0-8.6), intensive care unit admittance (OR = 4.5; CI = 1.2-14.2), and being placed on supplemental oxygen therapy (OR = 3.1; CI = 1.3-6.9). Individuals infected during their third trimester had higher mucosal anti-S IgG titers and lower viral RNA levels (P < 0.05) than those infected during their first or second trimesters. Pregnant individuals experiencing breakthrough infections due to the Omicron variant had reduced anti-S IgG compared to non-pregnant patients (P < 0.05). The observed increased severity of COVID-19 and reduced mucosal antibody responses particularly among pregnant participants infected with the Omicron variant suggest that maintaining high levels of SARS-CoV-2 immunity through booster vaccines may be important for the protection of this at-risk population.IMPORTANCEIn this retrospective observational cohort study, we analyzed remnant clinical samples from non-pregnant and pregnant individuals with confirmed severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infections who visited the Johns Hopkins Hospital System between October 2020 and May 2022. Disease severity, including intensive care unit admission, was greater among pregnant than non-pregnant patients. Vaccination reduced recovery of infectious virus and viral RNA levels in non-pregnant patients, but not in pregnant patients. In pregnant patients, increased nasopharyngeal viral RNA levels and recovery of infectious virus were associated with reduced mucosal IgG antibody responses, especially among women in their first trimester of pregnancy or experiencing breakthrough infections from Omicron variants. Taken together, this study provides insights into how pregnant patients are at greater risk of severe COVID-19. The novelty of this study is that it focuses on the relationship between the mucosal antibody response and its association with virus load and disease outcomes in pregnant people, whereas previous studies have focused on serological immunity. Vaccination status, gestational age, and SARS-CoV-2 omicron variant impact mucosal antibody responses and recovery of infectious virus from pregnant patients.
Keywords: COVID-19; Delta variant; Omicron variant; breakthrough infection; gestation.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Update of
-
Reduced control of SARS-CoV-2 infection is associated with lower mucosal antibody responses in pregnant women.medRxiv [Preprint]. 2023 Mar 20:2023.03.19.23287456. doi: 10.1101/2023.03.19.23287456. medRxiv. 2023. Update in: mSphere. 2024 Mar 26;9(3):e0081223. doi: 10.1128/msphere.00812-23. PMID: 36993216 Free PMC article. Updated. Preprint.
References
-
- Allotey J, Stallings E, Bonet M, Yap M, Chatterjee S, Kew T, Debenham L, Llavall AC, Dixit A, Zhou D, et al. 2020. Clinical manifestations, risk factors, and maternal and perinatal outcomes of coronavirus disease 2019 in pregnancy: living systematic review and meta-analysis. BMJ 370:m3320. doi: 10.1136/bmj.m3320 - DOI - PMC - PubMed
-
- Strid P, Zapata LB, Tong VT, Zambrano LD, Woodworth KR, Riser AP, Galang RR, Gilboa SM, Ellington SR. 2022. Coronavirus disease 2019 (COVID-19) severity among women of reproductive age with symptomatic laboratory-confirmed severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection by pregnancy status-United States, 1 January 2020-25 December 2021. Clin Infect Dis 75:S317–S325. doi: 10.1093/cid/ciac479 - DOI - PMC - PubMed
-
- Sherer ML, Lei J, Creisher PS, Jang M, Reddy R, Voegtline K, Olson S, Littlefield K, Park H-S, Ursin RL, Ganesan A, Boyer T, Elsayed N, Brown DM, Walch SN, Antar AAR, Manabe YC, Jones-Beatty K, Golden WC, Satin AJ, Sheffield JS, Pekosz A, Klein SL, Burd I. 2021. Pregnancy alters interleukin-1 beta expression and antiviral antibody responses during severe acute respiratory syndrome coronavirus 2 infection. Am J Obstet Gynecol 225:301. doi: 10.1016/j.ajog.2021.03.028 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
