

The Association Between National Institutes of Health Stroke Scale Score and Clinical Outcome in Patients with Large Core Infarctions Undergoing Endovascular Treatment
- PMID: 38427274
- PMCID: PMC11136902
- DOI: 10.1007/s40120-024-00588-8
The Association Between National Institutes of Health Stroke Scale Score and Clinical Outcome in Patients with Large Core Infarctions Undergoing Endovascular Treatment
Abstract
Introduction: This study aimed to analyze the association between baseline National Institutes of Health Stroke Scale (NIHSS) scores and clinical outcomes in patients with large core infarctions undergoing endovascular treatment (EVT), a relationship that remains unclear.
Methods: Data were obtained from the MAGIC study, a prospective multicenter cohort study focusing on patients with acute large core ischemic stroke. This analysis evaluated the impact of NIHSS scores on EVT outcomes in patients with large core infarctions. Primary outcome metrics included favorable outcomes (modified Rankin Scale [mRS] of 0-3 at 90 days), while secondary outcomes encompassed shifts in mRS scores, functional independence (mRS score of 0-2), mRS score of 0-4, and successful recanalization rates. Adverse events considered were symptomatic intracranial hemorrhage (sICH) and mortality.
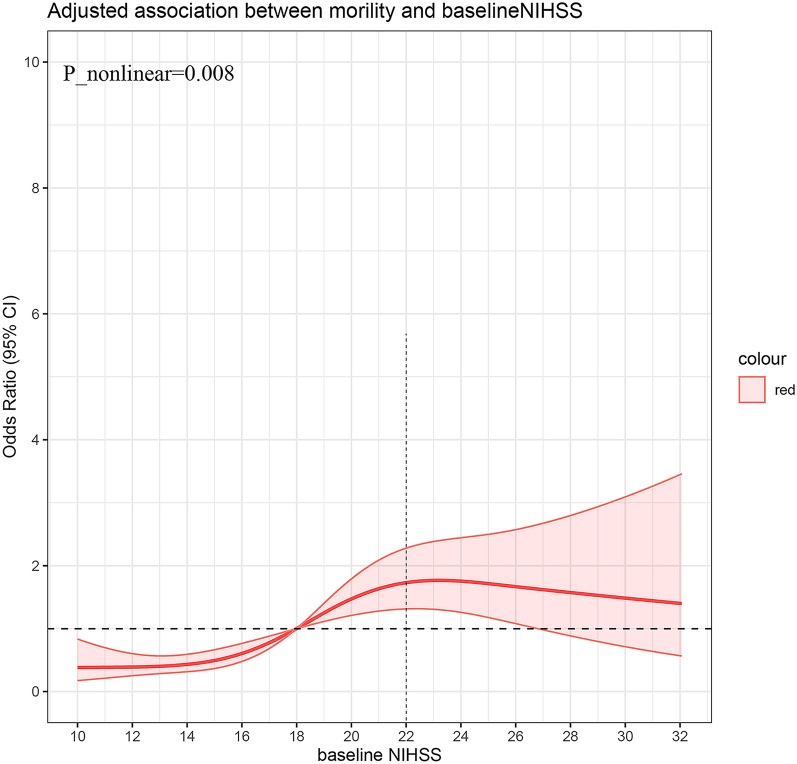
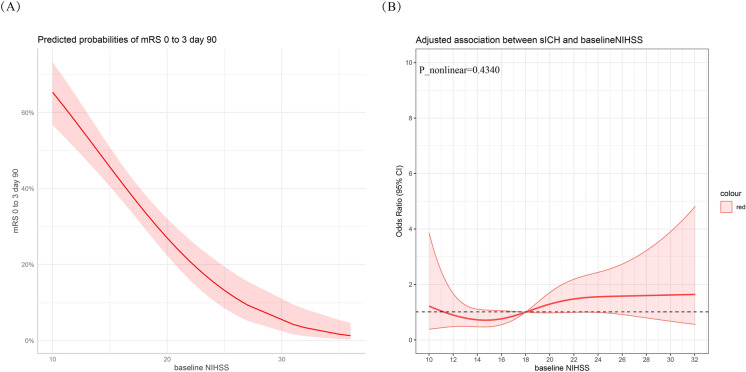
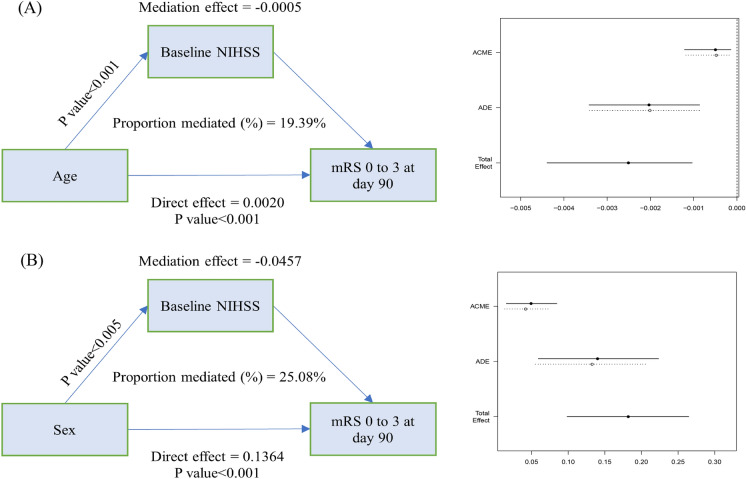
Results: A total of 490 patients were enrolled in this study. Higher baseline NIHSS scores were inversely correlated with favorable outcomes (adjusted odds ratio [OR] in model 3, 0.848 [0.797-0.903], P < 0.001), particularly in patients with NIHSS scores above 20 (adjusted OR in model 3, 0.518 [0.306-0.878] vs. 0.290 [0.161-0.523]). Regarding adverse events, higher baseline NIHSS scores significantly correlated with increased 90-day mortality rates (adjusted OR in model 3, 1.129 [1.072-1.189], P < 0.001). This correlation became insignificant when baseline NIHSS scores exceeded 22. Additionally, baseline NIHSS scores partially mediated the association between age (indirect effect = - 0.0005, 19.39% mediated) and sex (indirect effect = 0.0457, 25.08% mediated) with the primary outcome.
Conclusions: The findings indicate that higher baseline NIHSS scores correlate with poorer outcomes and increased mortality, particularly when scores exceed 20. Moreover, age and sex indirectly influence favorable outcomes through their association with baseline NIHSS scores.
Keywords: Endovascular therapy; Large core infarctions; National Institutes of Health Stroke Scale score.
© 2024. The Author(s).
Conflict of interest statement
Lingyu Zhang, Jinfu Ma, Mengmeng Wang, Lin Zhang, Wenzhe Sun, Honghong Ji, Chengsong Yue, Jiacheng Huang, Wenjie Zi, Fengli Li, Changwei Guo, Pengfei Wang have nothing to disclose.
Figures
Similar articles
-
Safety and outcomes of endovascular treatment in patients with very severe acute ischemic stroke.J Neurol. 2022 May;269(5):2493-2502. doi: 10.1007/s00415-021-10807-z. Epub 2021 Oct 7. J Neurol. 2022. PMID: 34618225
-
Safety and Outcome of Endovascular Treatment for Minor Ischemic Stroke: Results From the Multicenter Clinical Registry of Endovascular Treatment of Acute Ischemic Stroke in the Netherlands.J Stroke Cerebrovasc Dis. 2019 Mar;28(3):542-549. doi: 10.1016/j.jstrokecerebrovasdis.2018.10.029. Epub 2018 Dec 6. J Stroke Cerebrovasc Dis. 2019. PMID: 30527790
-
Outcomes of Endovascular Therapy in Acute Basilar Artery Occlusion With Severe Symptoms.JAMA Netw Open. 2021 Dec 1;4(12):e2139550. doi: 10.1001/jamanetworkopen.2021.39550. JAMA Netw Open. 2021. PMID: 34913974 Free PMC article.
-
Endovascular Thrombectomy VS. Medical Treatment for Mild Stroke Patients: A Systematic Review and Meta-Analysis.J Stroke Cerebrovasc Dis. 2020 Dec;29(12):105258. doi: 10.1016/j.jstrokecerebrovasdis.2020.105258. Epub 2020 Sep 25. J Stroke Cerebrovasc Dis. 2020. PMID: 32992178
-
Endovascular Therapy for Stroke Presenting Beyond 24 Hours: A Systematic Review and Meta-analysis.JAMA Netw Open. 2023 May 1;6(5):e2311768. doi: 10.1001/jamanetworkopen.2023.11768. JAMA Netw Open. 2023. PMID: 37140919 Free PMC article.
Cited by
-
Predictive outcome of late window ischemic stroke patients following endovascular therapy: a multi-center study.Front Neurol. 2025 Mar 27;16:1489714. doi: 10.3389/fneur.2025.1489714. eCollection 2025. Front Neurol. 2025. PMID: 40212610 Free PMC article.
-
Comparative Prognostic Value of the National Institutes of Health Stroke Scale (NIHSS) and the Glasgow Coma Scale (GCS) in Supratentorial and Infratentorial Stroke Patients in Western India.Cureus. 2024 Jul 30;16(7):e65778. doi: 10.7759/cureus.65778. eCollection 2024 Jul. Cureus. 2024. PMID: 39211638 Free PMC article.
-
Endovascular Treatment in Stroke Patients of Working Age: A Multicenter Observational Study of Real-World Outcomes.Ther Clin Risk Manag. 2025 Jul 5;21:1009-1019. doi: 10.2147/TCRM.S508295. eCollection 2025. Ther Clin Risk Manag. 2025. PMID: 40636546 Free PMC article.
References
Grants and funding
LinkOut - more resources
Full Text Sources
